

Variations in Multiple Birth Rates and Impact on Perinatal Outcomes in Europe
- PMID: 26930069
- PMCID: PMC4773186
- DOI: 10.1371/journal.pone.0149252
Variations in Multiple Birth Rates and Impact on Perinatal Outcomes in Europe
Abstract
Objective: Infants from multiple pregnancies have higher rates of preterm birth, stillbirth and neonatal death and differences in multiple birth rates (MBR) exist between countries. We aimed to describe differences in MBR in Europe and to investigate the impact of these differences on adverse perinatal outcomes at a population level.
Methods: We used national aggregate birth data on multiple pregnancies, maternal age, gestational age (GA), stillbirth and neonatal death collected in the Euro-Peristat project (29 countries in 2010, N = 5 074 643 births). We also used European Society of Human Reproduction and Embryology (ESHRE) data on assisted conception and single embryo transfer (SET). The impact of MBR on outcomes was studied using meta-analysis techniques with random-effects models to derive pooled risk ratios (pRR) overall and for four groups of country defined by their MBR. We computed population attributable risks (PAR) for these groups.
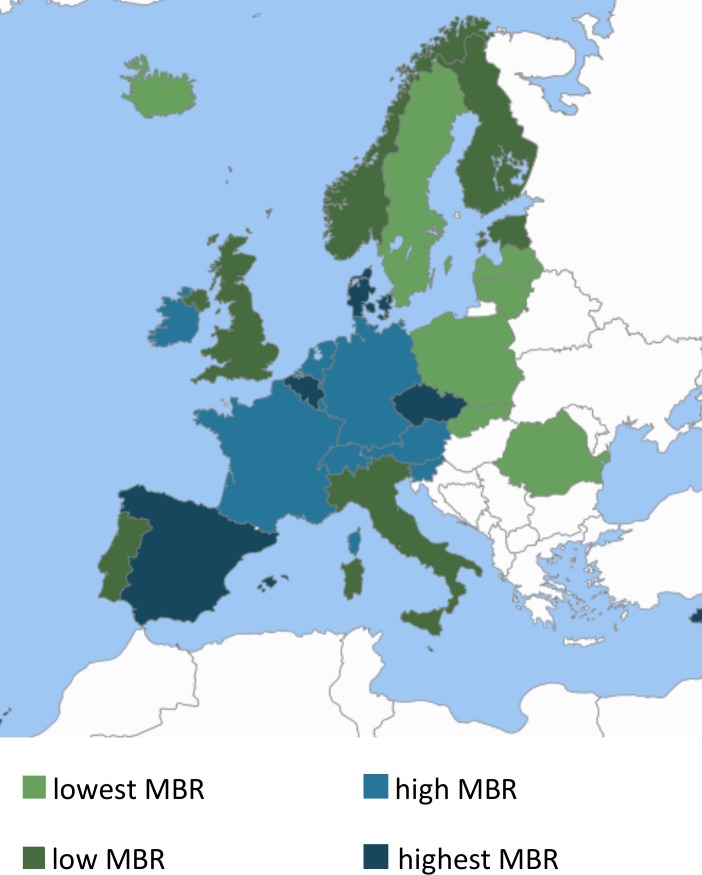
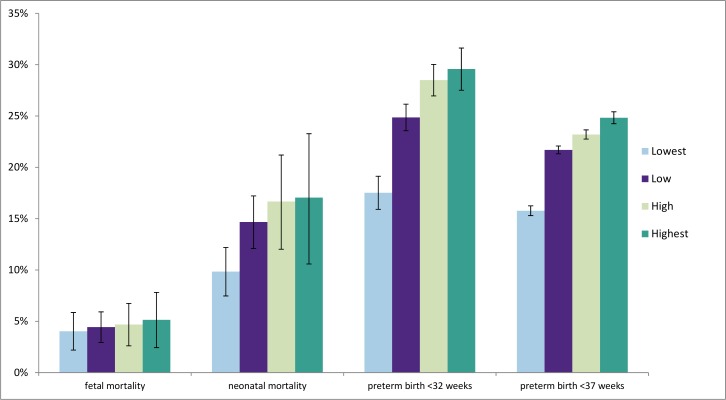
Results: In 2010, the average MBR was 16.8 per 1000 women giving birth, ranging from 9.1 (Romania) to 26.5 (Cyprus). Compared to singletons, multiples had a nine-fold increased risk (pRR 9.4, 95% Cl 9.1-9.8) of preterm birth (<37 weeks GA), an almost 12-fold increased risk (pRR 11.7, 95% CI 11.0-12.4) of very preterm birth (<32 weeks GA). Pooled RR were 2.4 (95% Cl 1.5-3.6) for fetal mortality at or after 28 weeks GA and 7.0 (95% Cl 6.1-8.0) for neonatal mortality. PAR of neonatal death and very preterm birth were higher in countries with high MBR compared to low MBR (17.1% (95% CI 13.8-20.2) versus 9.8% (95% Cl 9.6-11.0) for neonatal death and 29.6% (96% CI 28.5-30.6) versus 17.5% (95% CI 15.7-18.3) for very preterm births, respectively).
Conclusions: Wide variations in MBR and their impact on population outcomes imply that efforts by countries to reduce MBR could improve perinatal outcomes, enabling better long-term child health.
Conflict of interest statement
Figures
References
-
- Blondel B, Kaminski M. Trends in the occurrence, determinants, and consequences of multiple births. Seminars in perinatology 2002;26(4):239–49. - PubMed
-
- Tandberg A, Bjørge T, Børdahl PE, Skjaerven R. Increasing twinning rates in Norway, 1967–2004: the influence of maternal age and assisted reproductive technology (ART). Acta obstetricia et gynecologica Scandinavica 2007;86(7):833–9. - PubMed
-
- Sheay W, Ananth CV, Kinzler WL. Perinatal mortality in first- and second-born twins in the United States. Obstetrics and gynecology 2004;103(1):63–70. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
