

Comparative Epidemiology of Human Infections with Middle East Respiratory Syndrome and Severe Acute Respiratory Syndrome Coronaviruses among Healthcare Personnel
- PMID: 26930074
- PMCID: PMC4773072
- DOI: 10.1371/journal.pone.0149988
Comparative Epidemiology of Human Infections with Middle East Respiratory Syndrome and Severe Acute Respiratory Syndrome Coronaviruses among Healthcare Personnel
Abstract
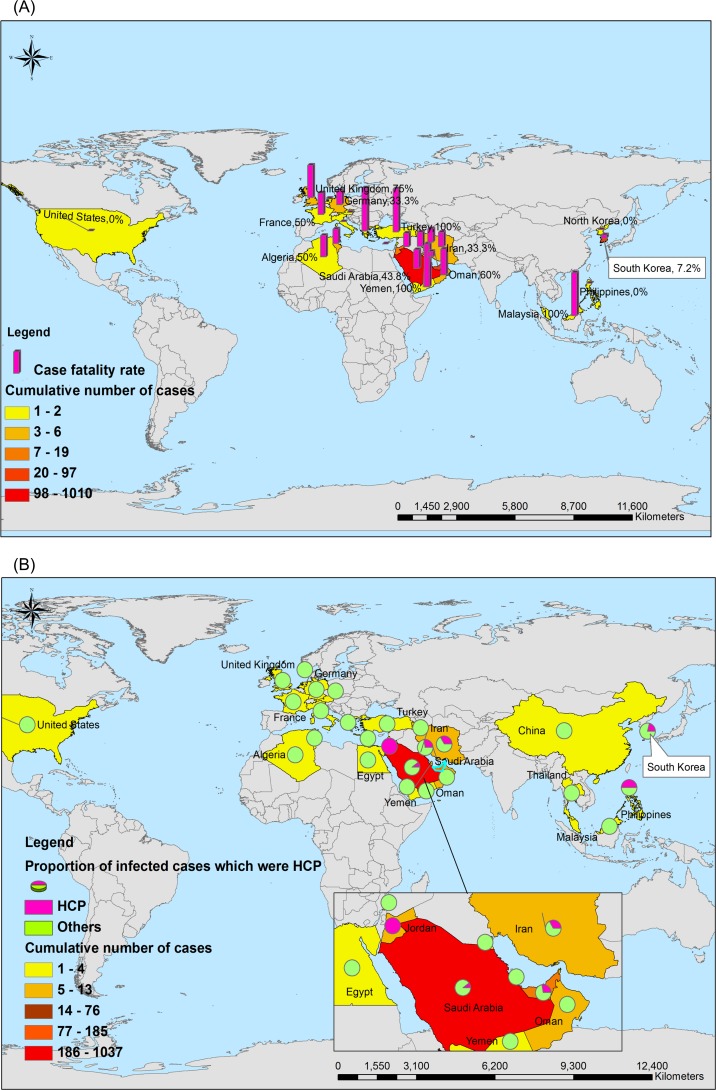
The largest nosocomial outbreak of Middle East respiratory syndrome (MERS) occurred in South Korea in 2015. Health Care Personnel (HCP) are at high risk of acquiring MERS-Coronavirus (MERS-CoV) infections, similar to the severe acute respiratory syndrome (SARS)-Coronavirus (SARS-CoV) infections first identified in 2003. This study described the similarities and differences in epidemiological and clinical characteristics of 183 confirmed global MERS cases and 98 SARS cases in Taiwan associated with HCP. The epidemiological findings showed that the mean age of MERS-HCP and total MERS cases were 40 (24~74) and 49 (2~90) years, respectively, much older than those in SARS [SARS-HCP: 35 (21~68) years, p = 0.006; total SARS: 42 (0~94) years, p = 0.0002]. The case fatality rates (CFR) was much lower in MERS-HCP [7.03% (9/128)] or SARS-HCP [12.24% (12/98)] than the MERS-non-HCP [36.96% (34/92), p<0.001] or SARS-non-HCP [24.50% (61/249), p<0.001], however, no difference was found between MERS-HCP and SARS-HCP [p = 0.181]. In terms of clinical period, the days from onset to death [13 (4~17) vs 14.5 (0~52), p = 0.045] and to discharge [11 (5~24) vs 24 (0~74), p = 0.010] and be hospitalized days [9.5 (3~22) vs 22 (0~69), p = 0.040] were much shorter in MERS-HCP than SARS-HCP. Similarly, days from onset to confirmation were shorter in MERS-HCP than MERS-non-HCP [6 (1~14) vs 10 (1~21), p = 0.044]. In conclusion, the severity of MERS-HCP and SARS-HCP was lower than that of MERS-non-HCP and SARS-non-HCP due to younger age and early confirmation in HCP groups. However, no statistical difference was found in MERS-HCP and SARS-HCP. Thus, prevention of nosocomial infections involving both novel Coronavirus is crucially important to protect HCP.
Conflict of interest statement
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
