

Vascular Endothelial Growth Factor and Podocyte Protection in Chronic Hypoxia: Effects of Endothelin-A Receptor Antagonism
- PMID: 26930122
- PMCID: PMC4828273
- DOI: 10.1159/000444719
Vascular Endothelial Growth Factor and Podocyte Protection in Chronic Hypoxia: Effects of Endothelin-A Receptor Antagonism
Abstract
Background: Podocytes are major components of the filtration barrier and a renal source of vascular endothelial growth factor (VEGF). Chronic renovascular disease (RVD) progressively degrades the renal function, accompanied by podocyte damage and a progressive reduction in VEGF. We showed that the endothelin (ET) pathway contributes to this pathological process and ET-A (but not ET-B) receptor antagonism protects the kidney in RVD. We hypothesize that ET-A-induced renoprotection is largely driven by the protection of podocyte integrity and function.
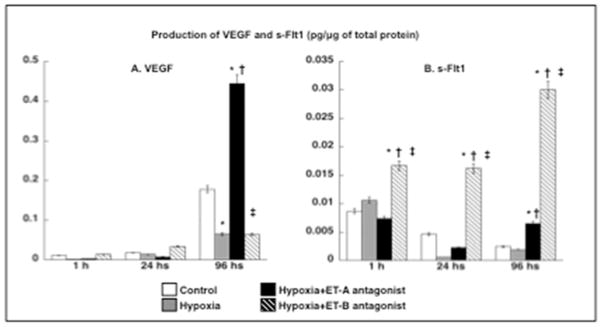
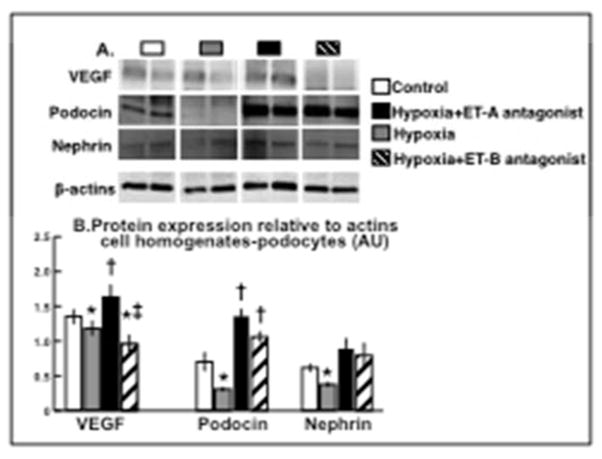
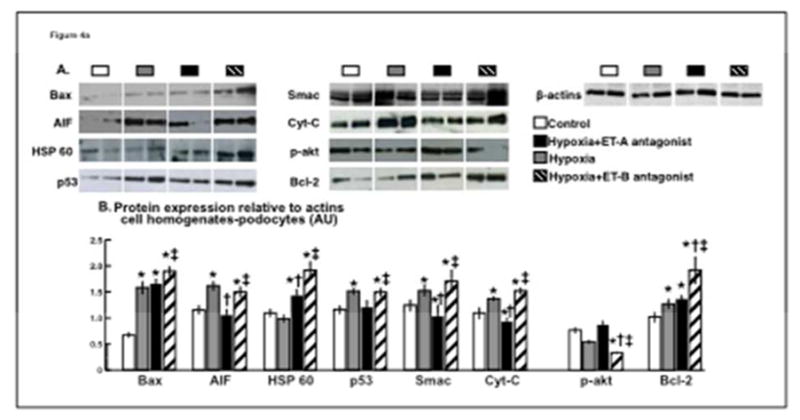
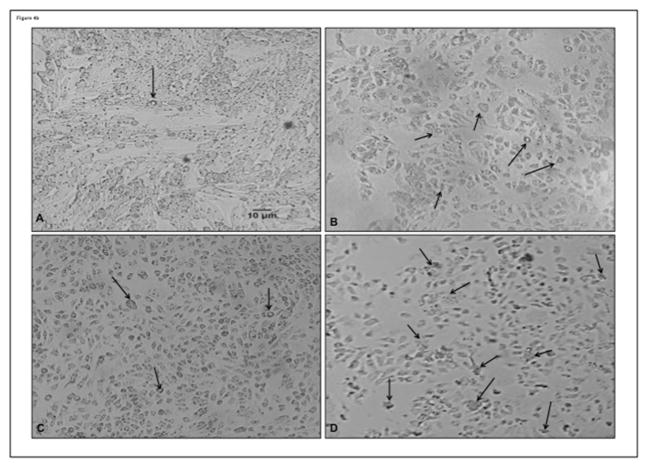
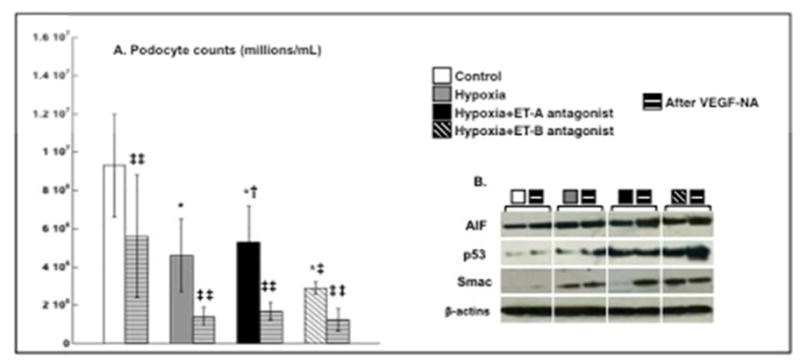
Methods: To mimic the renal environment of chronic RVD, human podocytes were incubated under chronic hypoxia for 96 h and divided in untreated or treated with an ET-A or ET-B receptor antagonist. Cells were quantified after 96 h. Cell homogenates and media were obtained after 1, 24 and 96 h to quantify production of VEGF, anti-VEGF soluble receptor s-Flt1, and the expression of apoptotic mediators. A separate set of similar experiments was performed after addition of a VEGF-neutralizing antibody (VEGF-NA).
Results: Hypoxia decreased podocyte number, which was exacerbated by ET-B but improved after ET-A antagonism. Production of VEGF was preserved by ET-A antagonism, whereas s-Flt1 increased in hypoxic cells after ET-B antagonism only, accompanied by a greater expression of pro-apoptotic mediators. On the other hand, treatment with VEGF-NA diminished ET-A-induced protection of podocytes.
Conclusion: ET-A antagonism preserves podocyte viability and integrity under chronic hypoxia, whereas ET-B antagonism exacerbates podocyte dysfunction and death. Enhanced bioavailability of VEGF after ET-A antagonism could be a pivotal mechanism of podocyte protection that significantly contributes to ET-A receptor blockade-induced renal recovery in chronic RVD.
© 2016 S. Karger AG, Basel.
Figures
Comment in
-
Life and Death of Podocytes: Not Only a Matter of Vascular Endothelial Growth Factor.Am J Nephrol. 2016;43(2):71-3. doi: 10.1159/000444723. Epub 2016 Mar 2. Am J Nephrol. 2016. PMID: 26930245 No abstract available.
References
-
- US Renal Data System U and Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States NIoH. National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2012.
-
- Vupputuri S, Kimes TM, Calloway MO, Christian JB, Bruhn D, Martin AA, Nichols GA. The economic burden of progressive chronic kidney disease among patients with type 2 diabetes. J Diabetes Complications. 2014;28:10–6. - PubMed
-
- Ritchie J, Green D, Chrysochou C, Chalmers N, Foley RN, Kalra PA. High-risk clinical presentations in atherosclerotic renovascular disease: prognosis and response to renal artery revascularization. Am J Kidney Dis. 2014;63:186–97. - PubMed
-
- Textor SC, Lerman LO. Reality and renovascular disease: when does renal artery stenosis warrant revascularization? Am J Kidney Dis. 2014;63:175–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
