

Comparing Tuberculosis Diagnostic Yield in Smear/Culture and Xpert® MTB/RIF-Based Algorithms Using a Non-Randomised Stepped-Wedge Design
- PMID: 26930400
- PMCID: PMC4773132
- DOI: 10.1371/journal.pone.0150487
Comparing Tuberculosis Diagnostic Yield in Smear/Culture and Xpert® MTB/RIF-Based Algorithms Using a Non-Randomised Stepped-Wedge Design
Abstract
Setting: Primary health services in Cape Town, South Africa.
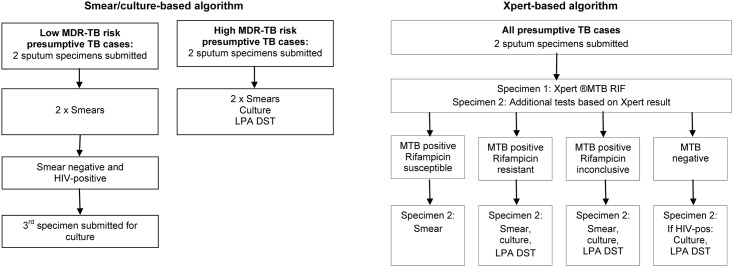
Study aim: To compare tuberculosis (TB) diagnostic yield in an existing smear/culture-based and a newly introduced Xpert® MTB/RIF-based algorithm.
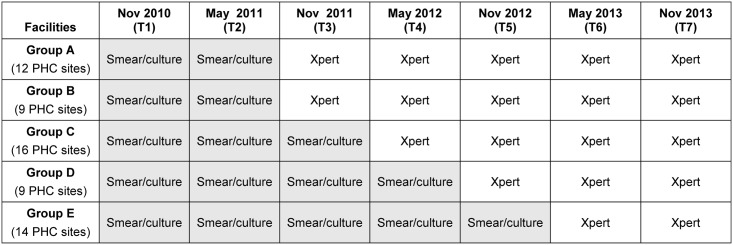
Methods: TB diagnostic yield (the proportion of presumptive TB cases with a laboratory diagnosis of TB) was assessed using a non-randomised stepped-wedge design as sites transitioned to the Xpert® based algorithm. We identified the full sequence of sputum tests recorded in the electronic laboratory database for presumptive TB cases from 60 primary health sites during seven one-month time-points, six months apart. Differences in TB yield and temporal trends were estimated using a binomial regression model.
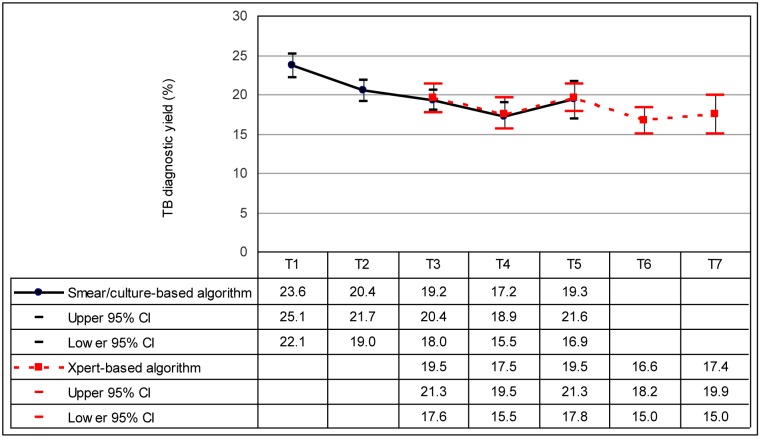
Results: TB yield was 20.9% (95% CI 19.9% to 22.0%) in the smear/culture-based algorithm compared to 17.9% (95%CI 16.4% to 19.5%) in the Xpert® based algorithm. There was a decline in TB yield over time with a mean risk difference of -0.9% (95% CI -1.2% to -0.6%) (p<0.001) per time-point. When estimates were adjusted for the temporal trend, TB yield was 19.1% (95% CI 17.6% to 20.5%) in the smear/culture-based algorithm compared to 19.3% (95% CI 17.7% to 20.9%) in the Xpert® based algorithm with a risk difference of 0.3% (95% CI -1.8% to 2.3%) (p = 0.796). Culture tests were undertaken for 35.5% of smear-negative compared to 17.9% of Xpert® negative low MDR-TB risk cases and for 82.6% of smear-negative compared to 40.5% of Xpert® negative high MDR-TB risk cases in respective algorithms.
Conclusion: Introduction of an Xpert® based algorithm did not produce the expected increase in TB diagnostic yield. Studies are required to assess whether improving adherence to the Xpert® negative algorithm for HIV-infected individuals will increase yield. In light of the high cost of Xpert®, a review of its role as a screening test for all presumptive TB cases may be warranted.
Conflict of interest statement
Figures
References
-
- World Health Organisation. Global Tuberculosis Report 2013. 2013.
-
- World Health Organisation. Automated Real-time Nucleic Acid Amplification Technology for Rapid and Simultaneous Detection of Tuberculosis and Rifampicin Resistance: Xpert MTB / RIF System. Policy Statement. 2011. - PubMed
-
- Meyer-Rath G, Schnippel K, Long L, MacLeod W, Sanne I, Stevens W, et al. The impact and cost of scaling up GeneXpert MTB/RIF in South Africa. PLoS One. 2012;7(5):e36966 Available from: http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0036966 [cited 2013 Feb 28] 10.1371/journal.pone.0036966 - DOI - PMC - PubMed
-
- Steingart KR, Sohn H, Schiller I, Kloda LA, Boehme CC, Pai M DN. Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults (Review). Cochrane Collaboration. 2013;(1). Available from: http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD009593.pub2/pdf/st... [cited 2013 Aug 11] - DOI - PMC - PubMed
-
- Mase SR, Ramsay A, Ng V, Henry M, Hopewell PC, Cunningham J, et al. Yield of serial sputum specimen examinations in the diagnosis of pulmonary tuberculosis: a systematic review. Int J Tuberc Lung Dis. 2007;11(5):485–95. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
