

Total Composite Flap Facelift and the Deep-Plane Transition Zone: A Critical Consideration in SMAS-Release Midface Lifting
- PMID: 26931306
- PMCID: PMC4827655
- DOI: 10.1093/asj/sjv250
Total Composite Flap Facelift and the Deep-Plane Transition Zone: A Critical Consideration in SMAS-Release Midface Lifting
Abstract
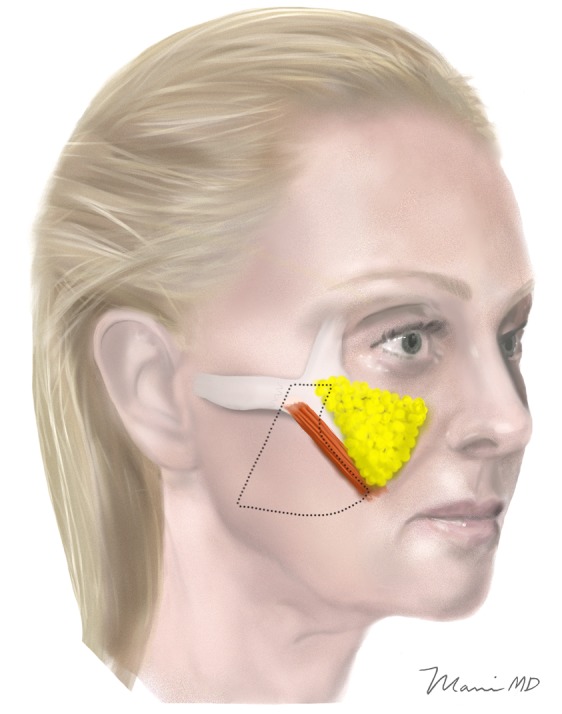
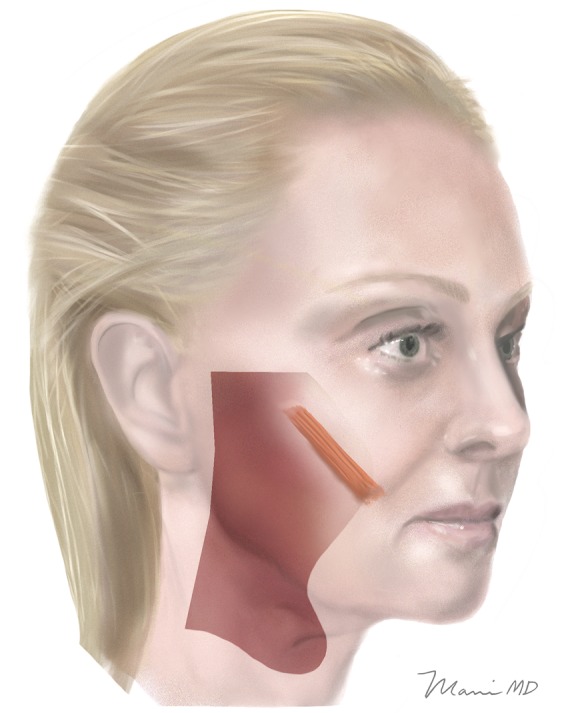
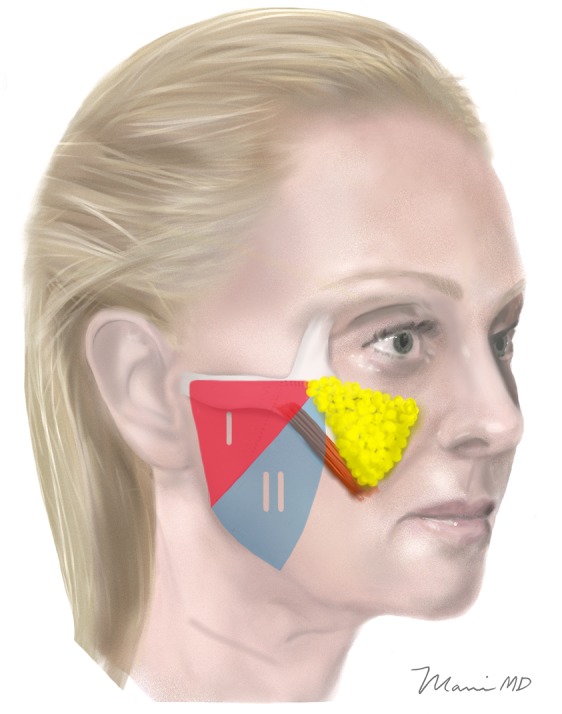
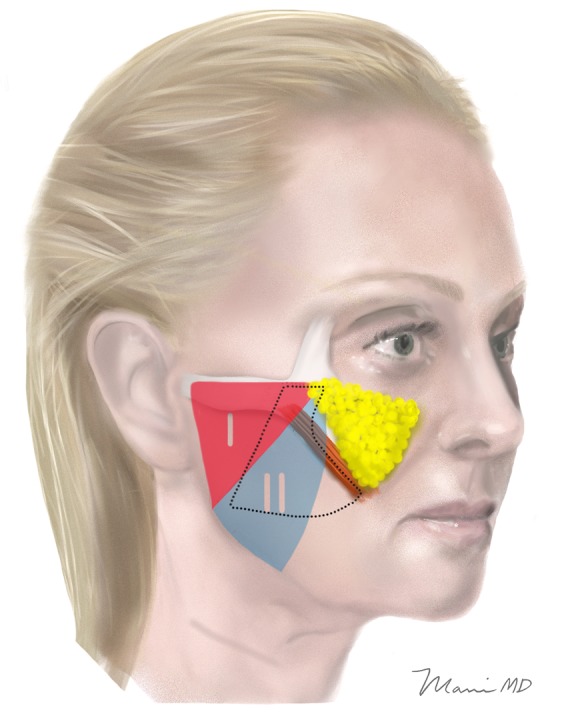
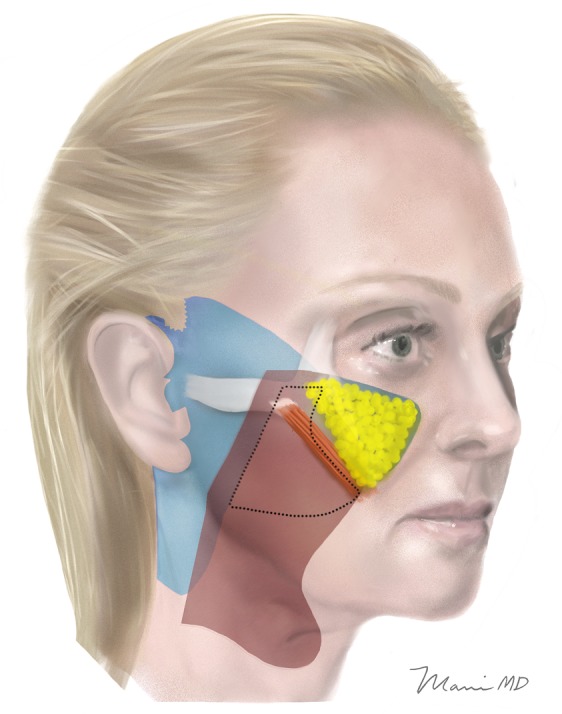
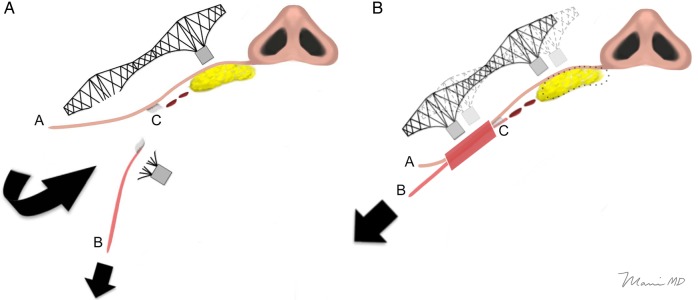
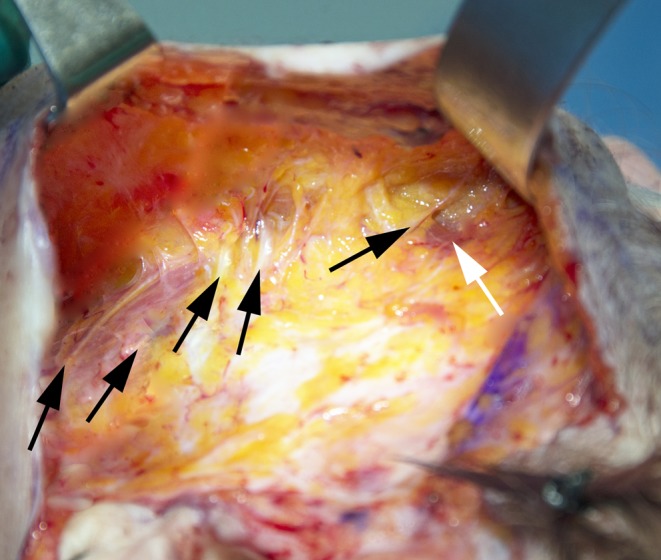
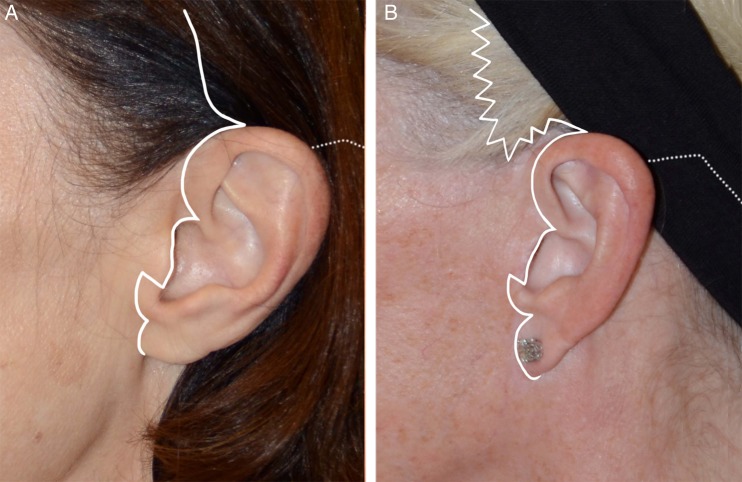
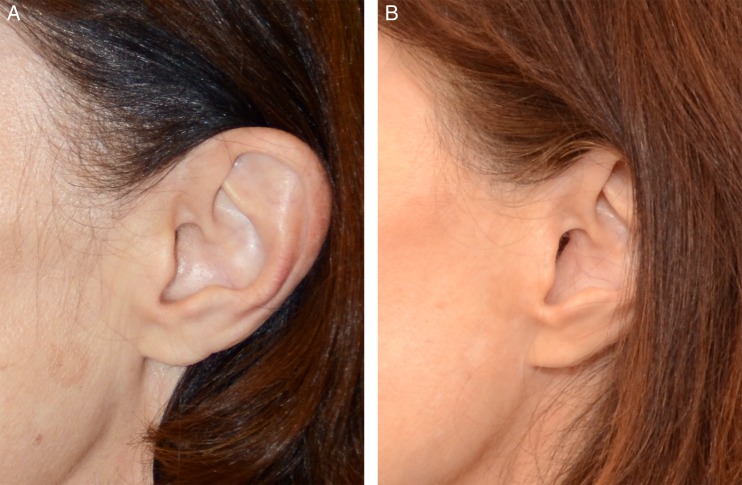
Background: Recent anatomic studies suggest the superficial musculoaponeurotic system (SMAS) layer attenuates in the midface. This led the author to switch from a bilamellar high SMAS dissection to a "total composite flap" technique, preserving skin and SMAS/platysma as one layer in a critical "deep-plane transition zone" (DTZ) lateral to the zygomaticus major muscle. This allows traction on the SMAS to translate to the malar fat pad via a "cantilever bridge" effect, which is lost when skin is undermined in the DTZ.
Objectives: This paper attempts to answer the question of whether the composite flap or bilamellar technique better lifts the midface, comparing groups where the DTZ was undermined: (1) only at a sub-SMAS level; or (2) at both subcutaneous and sub-SMAS levels.
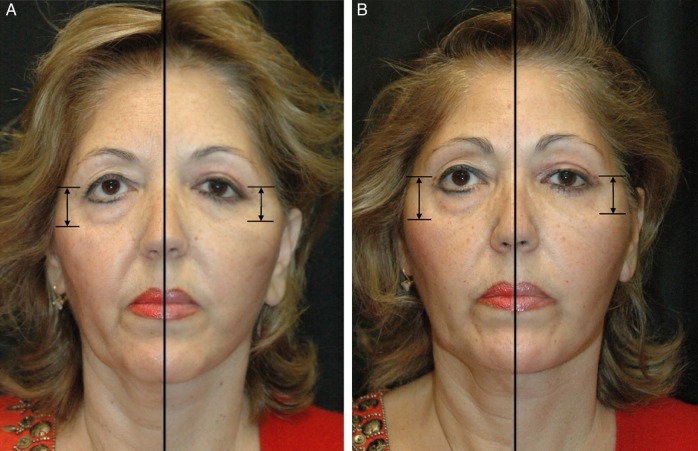
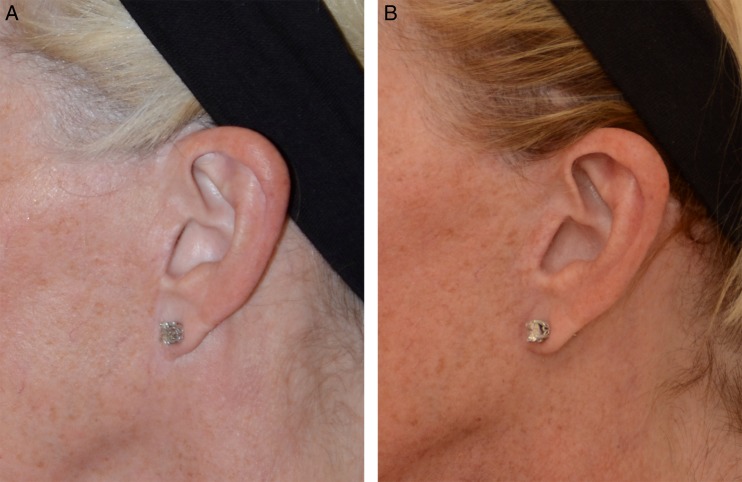
Methods: Thirty-five patients underwent bilamellar facelifts with skin and SMAS separated in the DTZ. Midfacial elevation was measured using size-matched preoperative and 18-month (average) postoperative photographs for the 70 hemi-midfaces. The same analysis was done for 35 patients undergoing total composite flap facelift, maintaining skin and SMAS as one layer in the DTZ. The two groups were compared.
Results: In the bilamellar group, the mean percentage of midfacial elevation at 18 months postoperative was 5.5% (range, 0.0%-17.8%). In the composite flap group, the percentage was 11.7% (range, 0.1%-32.3%). The difference was statistically significant.
Conclusions: Maintaining skin-SMAS attachments in the DTZ improves midface elevation during SMAS facelifting, exploiting a "cantilever bridge" effect of the skin transferring traction on the SMAS to the malar fat pad.
© 2016 The American Society for Aesthetic Plastic Surgery, Inc.
Figures


Comment in
-
Commentary on: Total Composite Flap Facelift and the Deep-Plane Transition Zone: A Critical Consideration in SMAS-Release Midface Lifting.Aesthet Surg J. 2016 May;36(5):546-9. doi: 10.1093/asj/sjw019. Epub 2016 Mar 1. Aesthet Surg J. 2016. PMID: 26931310 Free PMC article. No abstract available.
-
Response to "Commentary on: Total Composite Flap Facelift and the Deep-Plane Transition Zone: A Critical Consideration in SMAS-Release Midface Lifting".Aesthet Surg J. 2016 Jun;36(6):NP208-12. doi: 10.1093/asj/sjw057. Epub 2016 Mar 29. Aesthet Surg J. 2016. PMID: 27025246 Free PMC article. No abstract available.
Similar articles
-
A Novel Volumizing Extended Deep-Plane Facelift: Using Composite Flap Shifts to Volumize the Midface and Jawline.Facial Plast Surg Clin North Am. 2020 Aug;28(3):331-368. doi: 10.1016/j.fsc.2020.03.001. Facial Plast Surg Clin North Am. 2020. PMID: 32503718 Review.
-
Facelift Techniques: An Overview.Facial Plast Surg. 2022 Dec;38(6):540-545. doi: 10.1055/a-1877-9371. Epub 2022 Jun 16. Facial Plast Surg. 2022. PMID: 35709719
-
Is the SMAS Flap Facelift Safe? A Comparison of Complications Between the Sub-SMAS Approach Versus the Subcutaneous Approach With or Without SMAS Plication in Aesthetic Rhytidectomy at an Academic Institution.Aesthetic Plast Surg. 2015 Dec;39(6):870-6. doi: 10.1007/s00266-015-0558-9. Epub 2015 Aug 27. Aesthetic Plast Surg. 2015. PMID: 26311561
-
Modified Composite Plane Facelift with Extended Neck Dissection.Facial Plast Surg. 2022 Dec;38(6):584-592. doi: 10.1055/a-1862-9024. Epub 2022 May 26. Facial Plast Surg. 2022. PMID: 35617950
-
A Meta-Analysis of Complication Rates Among Different SMAS Facelift Techniques.Aesthet Surg J. 2019 Aug 22;39(9):927-942. doi: 10.1093/asj/sjz045. Aesthet Surg J. 2019. PMID: 30768122
Cited by
-
A Systematic Review and Meta-Analysis of Early Relapse After Facelift.Aesthetic Plast Surg. 2023 Feb;47(1):144-155. doi: 10.1007/s00266-022-02894-8. Epub 2022 May 9. Aesthetic Plast Surg. 2023. PMID: 35534779
-
Response to "Commentary on: Total Composite Flap Facelift and the Deep-Plane Transition Zone: A Critical Consideration in SMAS-Release Midface Lifting".Aesthet Surg J. 2016 Jun;36(6):NP208-12. doi: 10.1093/asj/sjw057. Epub 2016 Mar 29. Aesthet Surg J. 2016. PMID: 27025246 Free PMC article. No abstract available.
-
Commentary on: Total Composite Flap Facelift and the Deep-Plane Transition Zone: A Critical Consideration in SMAS-Release Midface Lifting.Aesthet Surg J. 2016 May;36(5):546-9. doi: 10.1093/asj/sjw019. Epub 2016 Mar 1. Aesthet Surg J. 2016. PMID: 26931310 Free PMC article. No abstract available.
-
Endoscopic, "Scarless" Composite Flap Face and Neck Lift.Facial Plast Surg. 2025 Feb;41(1):43-53. doi: 10.1055/a-2204-8798. Epub 2023 Nov 6. Facial Plast Surg. 2025. PMID: 37931912 Free PMC article.
References
-
- Connell BF, Semlacher RA. Contemporary deep layer facial rejuvenation. Plast Reconstr Surg. 1997;1006:1513-1523. - PubMed
-
- Marten TJ. High SMAS facelift: combined single flap lifting of the jawline, cheek, and midface. Clin Plast Surg. 2008;354:569-603. - PubMed
-
- Hamra ST. Composite rhytidectomy. Plast Reconstr Surg. 1992;901:1-13. - PubMed
-
- Skoog T. Plastic Surgery: New Methods and Refinements. Philadelphia: Saunders, 1974:1306-1342.
-
- Mendelson B. Facelift anatomy, SMAS retaining ligaments and facial spaces. In: Aston SJ, Steinbrech DS, Walden JL, eds. Aesthetic Plastic Surgery. London, UK: Saunders Elsevier; 2009:53-72.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
