

Tonsillectomy with Uvulopalatopharyngoplasty in Obstructive Sleep Apnea
- PMID: 26931522
- PMCID: PMC4746403
- DOI: 10.3238/arztebl.2016.0001
Tonsillectomy with Uvulopalatopharyngoplasty in Obstructive Sleep Apnea
Abstract
Background: Obstructive sleep apnea (OSA) is a very common disorder (prevalence 2-7% in women, 7-14% in men). It impairs the quality of life and increases mortality. Conservative treatment with continuous positive airway pressure is highly effective, but patient compliance is variable. Surgical treatments are controversial, as only a few are supported by evidence from controlled clinical trials.
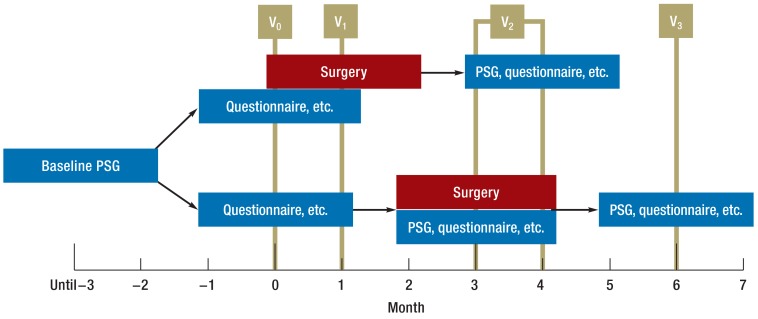
Methods: Adult patients with OSA, CPAP intolerance, and oropharyngeal obstruction were included in the trial. All underwent polysomnography (PSG) and were randomly allotted to one of two groups. Patients in the treatment group underwent tonsillectomy with uvulopalatopharyngoplasty (TE-UPPP) within one month. All patients had a follow-up PSG at three months, and all PSGs were evaluated in blinded fashion. The primary outcome variable was the apneahypopnea index (AHI) as determined by PSG. Other outcome variables were subjective symptoms (daytime sleepiness, quality of life), complications, and patient satisfaction.
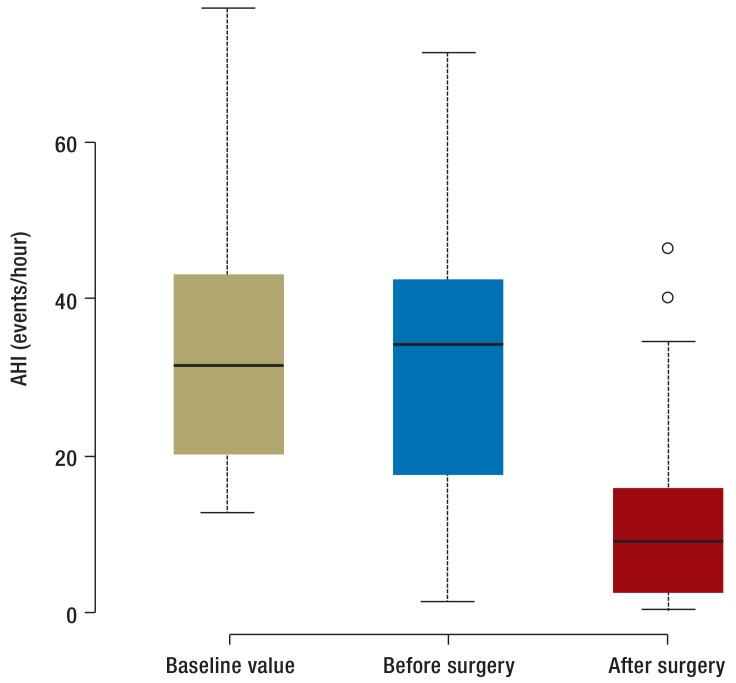
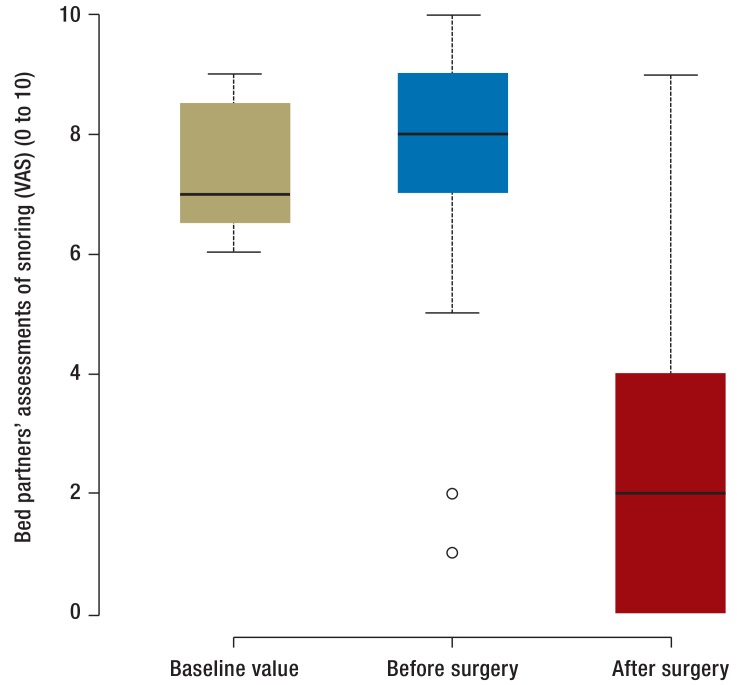
Results: 42 patents were included in the trial (23 in the treatment group, 19 in the control group). The baseline AHI was 35.7 ± 19.4/hr in the control group and 33.7 ± 14.6/hr in the treatment group. The corresponding figures at 3 months were 28.6 ± 19.4/hr in the control group and 15.4 ± 14.1/hr in the treatment group (p = 0.036). The intervention also led to significant improvement in daytime sleepiness and in snoring, according to the patients' and their bed partners' assessment. 97% of the patients who underwent surgery were satisfied with the outcome. 65% of them needed no further treatment for OSA.
Conclusion: TE-UPPP significantly improved apnea/hypopnea, daytime sleepiness, and snoring compared to control (i.e., no) treatment. It is a safe and effective treatment for OSA..
Figures
Comment in
-
Reasons for Refusal Were not Given.Dtsch Arztebl Int. 2016 Jul 11;113(27-28):484. doi: 10.3238/arztebl.2016.0484a. Dtsch Arztebl Int. 2016. PMID: 27476708 Free PMC article. No abstract available.
-
Further Long-term Studies Are Required.Dtsch Arztebl Int. 2016 Jul 11;113(27-28):484-5. doi: 10.3238/arztebl.2016.0484b. Dtsch Arztebl Int. 2016. PMID: 27476709 Free PMC article. No abstract available.
References
-
- Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med. 2002;165:1217–1239. - PubMed
-
- Wang X, Ouyang Y, Wang Z, Zhao G, Liu L, Bi Y. Obstructive sleep apnea and risk of cardiovascular disease and all-cause mortality: a meta-analysis of prospective cohort studies. International Journal of Cardiology. 2013;169:207–214. - PubMed
-
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046–1053. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical