

Intralymphatic mRNA vaccine induces CD8 T-cell responses that inhibit the growth of mucosally located tumours
- PMID: 26931556
- PMCID: PMC4773884
- DOI: 10.1038/srep22509
Intralymphatic mRNA vaccine induces CD8 T-cell responses that inhibit the growth of mucosally located tumours
Abstract
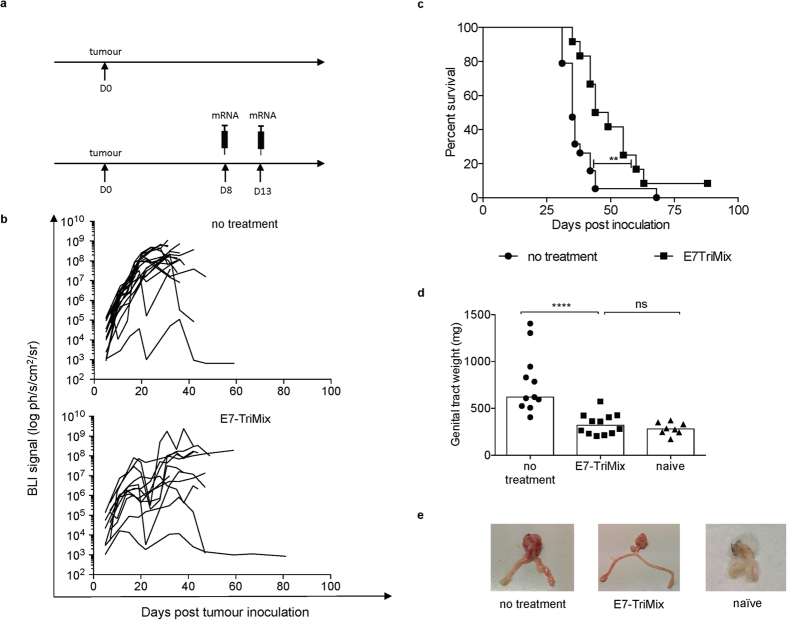
The lack of appropriate mouse models is likely one of the reasons of a limited translational success rate of therapeutic vaccines against cervical cancer, as rapidly growing ectopic tumours are commonly used for preclinical studies. In this work, we demonstrate that the tumour microenvironment of TC-1 tumours differs significantly depending on the anatomical location of tumour lesions (i.e. subcutaneously, in the lungs and in the genital tract). Our data demonstrate that E7-TriMix mRNA vaccine-induced CD8(+) T lymphocytes migrate into the tumour nest and control tumour growth, although they do not express mucosa-associated markers such as CD103 or CD49a. We additionally show that despite the presence of the antigen-specific T cells in the tumour lesions, the therapeutic outcomes in the genital tract model remain limited. Here, we report that such a hostile tumour microenvironment can be reversed by cisplatin treatment, leading to a complete regression of clinically relevant tumours when combined with mRNA immunization. We thereby demonstrate the necessity of utilizing clinically relevant models for preclinical evaluation of anticancer therapies and the importance of a simultaneous combination of anticancer immune response induction with targeting of tumour environment.
Conflict of interest statement
No patent was filed based on current study. The TriMix vaccine is however protected by patent on which K.T. is a co-inventor. The patent has been licensed to a biotech company. This company is not involved in current work or funding of this study. Other authors declare no conflict of interests.
Figures







Similar articles
-
Optimal induction of HPV DNA vaccine-induced CD8+ T cell responses and therapeutic antitumor effect by antigen engineering and electroporation.Vaccine. 2009 Sep 25;27(42):5906-12. doi: 10.1016/j.vaccine.2009.07.033. Epub 2009 Aug 3. Vaccine. 2009. PMID: 19651174
-
Induction of human papillomavirus oncogene-specific CD8 T-cell effector responses in the genital mucosa of vaccinated mice.Int J Cancer. 2010 May 15;126(10):2469-78. doi: 10.1002/ijc.24949. Int J Cancer. 2010. PMID: 19816937
-
Messenger RNA-based vaccines with dual activity induce balanced TLR-7 dependent adaptive immune responses and provide antitumor activity.J Immunother. 2011 Jan;34(1):1-15. doi: 10.1097/CJI.0b013e3181f7dbe8. J Immunother. 2011. PMID: 21150709
-
Tumour-derived IL-10 within tumour microenvironment represses the antitumour immunity of Socs1-silenced and sustained antigen expressing DCs.Eur J Cancer. 2012 Sep;48(14):2252-9. doi: 10.1016/j.ejca.2011.12.009. Epub 2012 Jan 7. Eur J Cancer. 2012. PMID: 22230748
-
Prophylactic and therapeutic efficacy of an attenuated Listeria monocytogenes-based vaccine delivering HPV16 E7 in a mouse model.Int J Mol Med. 2012 Dec;30(6):1335-42. doi: 10.3892/ijmm.2012.1136. Epub 2012 Sep 20. Int J Mol Med. 2012. PMID: 23027427
Cited by
-
The Delivery of mRNA Vaccines for Therapeutics.Life (Basel). 2022 Aug 17;12(8):1254. doi: 10.3390/life12081254. Life (Basel). 2022. PMID: 36013433 Free PMC article. Review.
-
Formulation and Delivery Technologies for mRNA Vaccines.Curr Top Microbiol Immunol. 2022;440:71-110. doi: 10.1007/82_2020_217. Curr Top Microbiol Immunol. 2022. PMID: 32483657 Free PMC article.
-
Tissue-specific tumour microenvironments are an emerging determinant of immunotherapy responses.J Thorac Dis. 2020 Aug;12(8):4504-4509. doi: 10.21037/jtd.2020.03.64. J Thorac Dis. 2020. PMID: 32944364 Free PMC article. No abstract available.
-
Immune-related dissociated response as a specific atypical response pattern in solid tumors with immune checkpoint blockade.Ther Adv Med Oncol. 2022 May 6;14:17588359221096877. doi: 10.1177/17588359221096877. eCollection 2022. Ther Adv Med Oncol. 2022. PMID: 35547094 Free PMC article.
-
mRNA - A game changer in regenerative medicine, cell-based therapy and reprogramming strategies.Adv Drug Deliv Rev. 2021 Dec;179:114002. doi: 10.1016/j.addr.2021.114002. Epub 2021 Oct 13. Adv Drug Deliv Rev. 2021. PMID: 34653534 Free PMC article. Review.
References
-
- Ferlay J. et al.. Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11. Globocan 2012 v1.0 (2013). at < http://globocan.iarc.fr > .
-
- Bosetti C., Turati F. & La Vecchia C. Hepatocellular carcinoma epidemiology. Best Pract. Res. Clin. Gastroenterol. 28, 753–70 (2014). - PubMed
-
- Hopkins T. G. & Wood N. Female human papillomavirus (HPV) vaccination: global uptake and the impact of attitudes. Vaccine 31, 1673–9 (2013). - PubMed
-
- Tabrizi S. N. et al.. Assessment of herd immunity and cross-protection after a human papillomavirus vaccination programme in Australia: a repeat cross-sectional study. Lancet. Infect. Dis. 14, 958–66 (2014). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
