

Comparison of serological methods with PCR-based methods for the diagnosis of community-acquired pneumonia caused by atypical bacteria
- PMID: 26932735
- PMCID: PMC4774004
- DOI: 10.1186/s12952-016-0047-y
Comparison of serological methods with PCR-based methods for the diagnosis of community-acquired pneumonia caused by atypical bacteria
Abstract
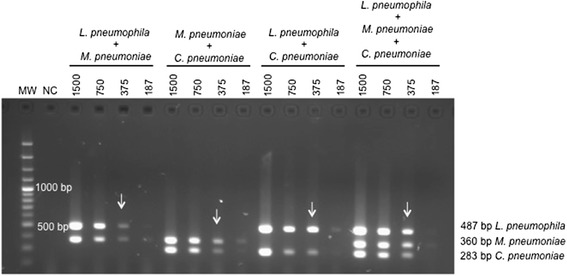
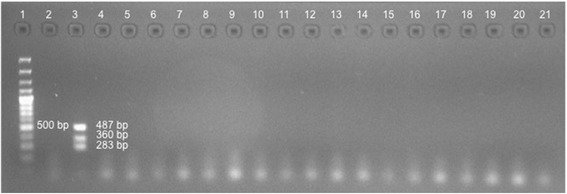
Background: The diagnosis of community-acquired pneumonia (CAP) caused by Legionella pneumophila, Mycoplasma pneumoniae, and Chlamydophila pneumoniae is traditionally based on cultures and serology, which have special requirements, are time-consuming, and offer delayed results that limit their clinical usefulness of these techniques. We sought to develop a multiplex PCR (mPCR) method to diagnosis these bacterial infections in CAP patients and to compare the diagnostic yields obtained from mPCR of nasopharyngeal aspirates (NPAs), nasopharyngeal swabs (NPSs), and induced sputum (IS) with those obtained with specific PCR commercial kits, paired serology, and urinary antigen.
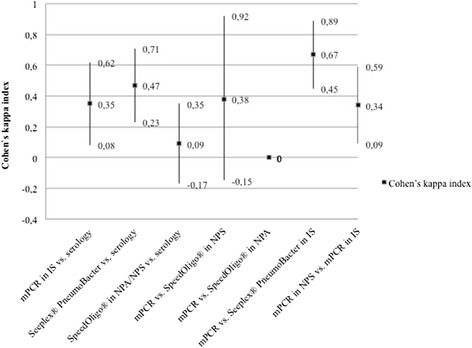
Results: A total of 225 persons were included. Of these, 10 patients showed serological evidence of L. pneumophila infection, 30 of M. pneumoniae, and 18 of C. pneumoniae; 20 individuals showed no CAP. The sensitivities were mPCR-NPS = 23.1%, mPCR-IS = 57.1%, Seeplex®-IS = 52.4%, and Speed-oligo®-NPA/NPS = 11.1%, and the specificities were mPCR-NPS = 97.1%, mPCR-IS = 77.8%, Seeplex®-IS = 92.6%, and Speed-oligo®-NPA/NPS = 96.1%. The concordance between tests was poor (kappa <0.4), except for the concordance between mPCR and the commercial kit in IS (0.67). In individuals with no evidence of CAP, positive reactions were observed in paired serology and in all PCRs.
Conclusions: All PCRs had good specificity but low sensitivity in nasopharyngeal samples. The sensitivity of mPCR and Seeplex® in IS was approximately 60%; thus, better diagnostic techniques for these three bacteria are required.
Figures
Similar articles
-
Single tube real time PCR for detection of Streptococcus pneumoniae, Mycoplasma pneumoniae, Chlamydophila pneumoniae and Legionella pneumophila from clinical samples of CAP.Acta Microbiol Immunol Hung. 2012 Jun;59(2):171-84. doi: 10.1556/AMicr.59.2012.2.3. Acta Microbiol Immunol Hung. 2012. PMID: 22750778
-
Comparison of sputum and nasopharyngeal swab specimens for molecular diagnosis of Mycoplasma pneumoniae, Chlamydophila pneumoniae, and Legionella pneumophila.Ann Lab Med. 2012 Mar;32(2):133-8. doi: 10.3343/alm.2012.32.2.133. Epub 2012 Feb 23. Ann Lab Med. 2012. PMID: 22389880 Free PMC article.
-
Diagnosis of atypical pathogens in patients hospitalized with community-acquired respiratory infection.Scand J Infect Dis. 2004;36(4):269-73. doi: 10.1080/00365540410020127. Scand J Infect Dis. 2004. PMID: 15198183
-
[The role of atypical pathogen: Mycoplasma pneumoniae and Chlamydia pneumoniae in the acute respiratory infection in childhood].Jpn J Antibiot. 2000 Jun;53 Suppl B:13-21. Jpn J Antibiot. 2000. PMID: 12572086 Review. Japanese.
-
Where is Chlamydophila pneumoniae pneumonia?Respir Investig. 2020 Sep;58(5):336-343. doi: 10.1016/j.resinv.2020.06.002. Epub 2020 Jul 20. Respir Investig. 2020. PMID: 32703757
Cited by
-
Community-acquired pneumonia related to intracellular pathogens.Intensive Care Med. 2016 Sep;42(9):1374-86. doi: 10.1007/s00134-016-4394-4. Epub 2016 Jun 8. Intensive Care Med. 2016. PMID: 27276986 Review.
-
Are ELISA and PCR Discrepancies in the Identification of Chlamydia pneumoniae Caused by the Presence of "Chlamydia-Related Bacteria"?Microorganisms. 2023 Jan 11;11(1):187. doi: 10.3390/microorganisms11010187. Microorganisms. 2023. PMID: 36677479 Free PMC article.
-
Viral and bacterial coinfection among hospitalized children with respiratory tract infections.Am J Infect Control. 2020 Oct;48(10):1231-1236. doi: 10.1016/j.ajic.2020.01.013. Epub 2020 Feb 26. Am J Infect Control. 2020. PMID: 32113661 Free PMC article.
-
Reliable and Sensitive Nested PCR for the Detection of Chlamydia in Sputum.Microorganisms. 2021 Apr 27;9(5):935. doi: 10.3390/microorganisms9050935. Microorganisms. 2021. PMID: 33925646 Free PMC article.
-
Epidemiological and Clinical Characteristics of Respiratory Syncytial Virus Infections in Children Aged <5 Years in China, from 2014−2018.Vaccines (Basel). 2022 May 20;10(5):810. doi: 10.3390/vaccines10050810. Vaccines (Basel). 2022. PMID: 35632566 Free PMC article.
References
-
- Donalisio MR, Arca CHM, de Madureira PR. Clinical, epidemiological, and etiological profile of inpatients with community-acquired pneumonia at a general hospital in the Sumaré microregion of Brazil. J Bras Pneumol Publicaça̋o Of Soc Bras Pneumol E Tisilogia. 2011;37:200–8. doi: 10.1590/S1806-37132011000200010. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
