

Does Teriparatide Improve Femoral Neck Fracture Healing: Results From A Randomized Placebo-controlled Trial
- PMID: 26932738
- PMCID: PMC4814417
- DOI: 10.1007/s11999-015-4669-z
Does Teriparatide Improve Femoral Neck Fracture Healing: Results From A Randomized Placebo-controlled Trial
Abstract
Background: There is a medical need for therapies that improve hip fracture healing. Teriparatide (Forteo(®)/ Forsteo(®), recombinant human parathyroid hormone) is a bone anabolic drug that is approved for treatment of osteoporosis and glucocorticoid-induced osteoporosis in men and postmenopausal women at high fracture risk. Preclinical and preliminary clinical data also suggest that teriparatide may enhance bone healing.
Questions/purposes: We wished to test the hypotheses that treatment with teriparatide versus placebo would improve femoral neck fracture healing after internal fixation as measured by (1) frequency of revision surgery, (2) radiographic fracture healing, and (3) other outcomes including pain control, gait speed, and safety.
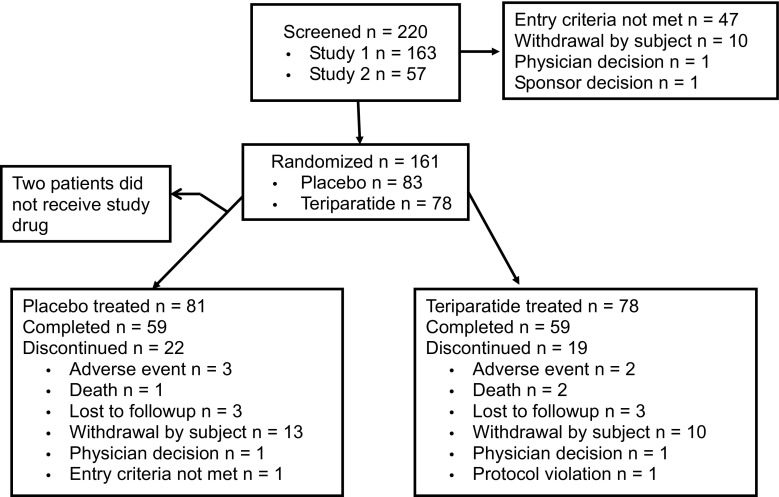
Methods: We initiated two separate, but identically designed, clinical trials to meet FDA requirements to provide substantial evidence to support approval of a new indication. The two prospective, randomized double-blind, placebo-controlled Phase III studies were designed to evaluate the effect of subcutaneous teriparatide (20 μg/day) for 6 months versus placebo on fracture healing at 24 months. The trials were conducted concurrently with a planned enrollment of 1220 patients per trial. However, enrollment was stopped owing to very slow patient accrual, and an a priori decision was made to pool the results of those studies for statistical analyses before study completion; pooling was specified in both protocols. Randomization was stratified by fixation (sliding hip screw or multiple cancellous screws) and fracture type (displaced or nondisplaced). An independent Central Adjudication Committee reviewed revision surgical procedures and radiographs. A total of 159 patients were randomized in the two trials (81 placebo, 78 teriparatide). The combined program had very low power to detect the originally expected treatment effect but had approximately 80% power to detect a larger difference of 12% between treatment groups for risk of revision surgery.
Results: The proportion of patients undergoing revision surgery at 12 months was 14% (11 of 81) in the placebo group versus 17% (13 of 78) in the teriparatide group. Central Adjudication Committee review excluded two of these patients treated with placebo from the primary analysis. After exclusions, the proportion of patients who did not undergo revision surgery at 12 months (primary endpoint) was not different between the study and placebo groups, at 88% in the placebo group (90% CI, 0.79-0.93) versus 84% in the teriparatide group (90% CI, 0.75-0.90; p = 0.743). There also were no differences between groups in the proportion of patients achieving radiographic fracture healing at 12 months (75% [61 of 81] placebo versus 73% [57 of 78] teriparatide; odds ratio, 0.89; 90% CI, 0.46-1.72; p = 0.692) or in measures of pain control (such as pain during ambulation, 92% [55 of 62] placebo versus 91% [52 of 57] teriparatide; odds ratio, 0.91; 90% CI, 0.25-3.37; p = 0.681). The frequency of patients reporting adverse events was 49% [40 of 81] in the placebo group versus 45% [35 of 78] in the teriparatide group (p = 0.634) during the 6-month treatment period.
Conclusions: The small sample size limited this study's power to detect potential differences, and the results are exploratory. With the patients available, teriparatide did not decrease the risk of revision surgery, improve radiographic signs of fracture healing, or decrease pain compared with the placebo. The adverse event data observed were consistent with the teriparatide safety profile. Functional and health outcome data from the studies may help improve our understanding of patients recovering from femoral neck fractures. Further large controlled studies are required to determine the effect of teriparatide on fracture healing.
Level of evidence: Level II, prospective study.
Figures
Comment in
-
CORR Insights(®): Does Teriparatide Improve Femoral Neck Fracture Healing: Results From A Randomized Placebo-controlled Trial.Clin Orthop Relat Res. 2016 May;474(5):1245-6. doi: 10.1007/s11999-016-4778-3. Epub 2016 Mar 11. Clin Orthop Relat Res. 2016. PMID: 26968724 Free PMC article. No abstract available.
Similar articles
-
CORR Insights(®): Does Teriparatide Improve Femoral Neck Fracture Healing: Results From A Randomized Placebo-controlled Trial.Clin Orthop Relat Res. 2016 May;474(5):1245-6. doi: 10.1007/s11999-016-4778-3. Epub 2016 Mar 11. Clin Orthop Relat Res. 2016. PMID: 26968724 Free PMC article. No abstract available.
-
The Radiographic Union Score for Hip (RUSH) Identifies Radiographic Nonunion of Femoral Neck Fractures.Clin Orthop Relat Res. 2016 Jun;474(6):1396-404. doi: 10.1007/s11999-015-4680-4. Clin Orthop Relat Res. 2016. PMID: 26728521 Free PMC article.
-
Effect of Abaloparatide vs Placebo on New Vertebral Fractures in Postmenopausal Women With Osteoporosis: A Randomized Clinical Trial.JAMA. 2016 Aug 16;316(7):722-33. doi: 10.1001/jama.2016.11136. JAMA. 2016. PMID: 27533157 Clinical Trial.
-
Use of teriparatide in osteoporotic fracture patients.Injury. 2016 Jan;47 Suppl 1:S36-8. doi: 10.1016/S0020-1383(16)30009-2. Injury. 2016. PMID: 26768289 Review.
-
Accelerated fracture healing with teriparatide.Arq Bras Endocrinol Metabol. 2013 Mar;57(2):153-6. doi: 10.1590/s0004-27302013000200010. Arq Bras Endocrinol Metabol. 2013. PMID: 23525295 Review.
Cited by
-
Assessment of evidence for the off-label application of osteoanabolic drugs in fracture healing and spinal fusion.J Bone Miner Metab. 2025 Mar;43(2):57-60. doi: 10.1007/s00774-025-01589-9. Epub 2025 Feb 18. J Bone Miner Metab. 2025. PMID: 39964554 Review.
-
Present and future scope of recombinant parathyroid hormone therapy in orthopaedics.J Clin Orthop Trauma. 2021 Feb 7;17:54-58. doi: 10.1016/j.jcot.2021.01.019. eCollection 2021 Jun. J Clin Orthop Trauma. 2021. PMID: 33717971 Free PMC article. Review.
-
Teriparatide and stress fracture healing in young adults (RETURN - Research on Efficacy of Teriparatide Use in the Return of recruits to Normal duty): study protocol for a randomised controlled trial.Trials. 2021 Aug 30;22(1):580. doi: 10.1186/s13063-021-05556-3. Trials. 2021. PMID: 34461961 Free PMC article.
-
The effect of intermittent parathyroid hormone on bone lengthening: current evidence to inform future effective interventions.Osteoporos Int. 2023 Oct;34(10):1657-1675. doi: 10.1007/s00198-023-06809-4. Epub 2023 Jun 8. Osteoporos Int. 2023. PMID: 37286663 Review.
-
Post-surgery interventions for hip fracture: a systematic review of randomized controlled trials.BMC Musculoskelet Disord. 2023 May 25;24(1):417. doi: 10.1186/s12891-023-06512-9. BMC Musculoskelet Disord. 2023. PMID: 37231406 Free PMC article.
References
-
- Aspenberg P, Genant HK, Johansson T, Nino AJ, See K, Krohn K, García-Hernández PA, Recknor CP, Einhorn TA, Dalsky GP, Mitlak BH, Fierlinger A, Lakshmanan MC. Teriparatide for acceleration of fracture repair in humans: a prospective, randomized, double-blind study of 102 postmenopausal women with distal radial fractures. J Bone Miner Res. 2010;25:404–414. doi: 10.1359/jbmr.090731. - DOI - PubMed
-
- Bassler D, Briel M, Montori VM, Lane M, Glasziou P, Zhou Q, Heels-Ansdell D, Walter SD, Guyatt GH; STOPIT-2 Study Group, Flynn DN, Elamin MB, Murad MH, Abu Elnour NO, Lampropulos JF, Sood A, Mullan RJ, Erwin PJ, Bankhead CR, Perera R, Ruiz Culebro C, You JJ, Mulla SM, Kaur J, Nerenberg KA, Schünemann H, Cook DJ, Lutz K, Ribic CM, Vale N, Malaga G, Akl EA, Ferreira-Gonzalez I, Alonso-Coello P, Urrutia G, Kunz R, Bucher HC, Nordmann AJ, Raatz H, da Silva SA, Tuche F, Strahm B, Djulbegovic B, Adhikari NK, Mills EJ, Gwadry-Sridhar F, Kirpalani H, Soares HP, Karanicolas PJ, Burns KE, Vandvik PO, Coto-Yglesias F, Chrispim PP, Ramsay T. Stopping randomized trials early for benefit and estimation of treatment effects: systematic review and meta-regression analysis. JAMA. 2010;303:1180–1187. - PubMed
-
- Bhandari M, Devereaux PJ, Swiontkowski MF, Tornetta P, 3rd, Obremskey W, Koval KJ, Nork S, Sprague S, Schemitsch EH, Guyatt GH. Internal fixation compared with arthroplasty for displaced fractures of the femoral neck: a meta-analysis. J Bone Joint Surg Am. 2003;85:1673–1681. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
