

No Decrease in Early Ventilator-Associated Pneumonia After Early Use of Chlorhexidine
- PMID: 26932921
- PMCID: PMC5301802
- DOI: 10.4037/ajcc2016823
No Decrease in Early Ventilator-Associated Pneumonia After Early Use of Chlorhexidine
Abstract
Background: Oral chlorhexidine prophylaxis can decrease occurrence of ventilator-associated pneumonia. However, the importance of timing has never been fully explored.
Objective: To see if early administration of oral chlorhexidine is associated with lower incidence of early ventilator-associated pneumonia (within 5 days of admission to intensive care unit) in intubated air ambulance patients.
Methods: A single-center, retrospective cohort study of intubated adults transported by a university-based air ambulance service and admitted to a surgical intensive care unit from July 2011 through April 2013. Primary exposure was time from helicopter retrieval to the first dose of oral chlorhexidine in the intensive care unit. Early chlorhexidine was defined as receipt of the drug within 6 hours of helicopter departure. The primary outcome was clinical diagnosis of early ventilator-associated pneumonia. Patients who were less than 18 years old, died within 72 hours of admission, or had pneumonia at admission were excluded.
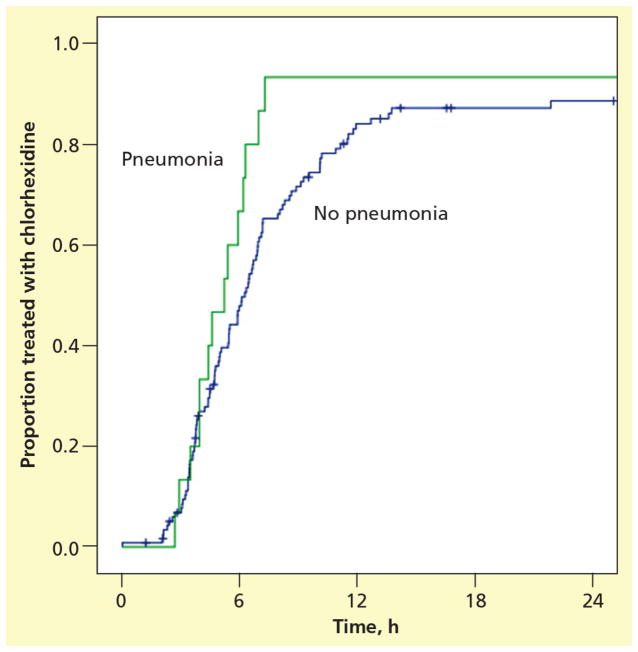
Results: Among 134 patients, 49% were treated with chlorhexidine before 6 hours, 84% were treated before 12 hours, and 11% were treated for early pneumonia. Early chlorhexidine (before 6 hours; 15%) was not associated (P = .21) with early pneumonia (8%). Furthermore, median times to chlorhexidine did not differ significantly (P = .23) between patients in whom pneumonia developed (5.2 hours) and patients with no pneumonia (6.1 hours).
Conclusions: Early administration of oral chlorhexidine in intubated patients was not associated with a reduction in the incidence of ventilator-associated pneumonia in a surgical intensive care unit with high rates of chlorhexidine administration before 12 hours.
©2016 American Association of Critical-Care Nurses.
Figures
Similar articles
-
Prehospital oral chlorhexidine does not reduce the rate of ventilator-associated pneumonia among critically ill trauma patients: A prospective concurrent-control study.J Crit Care. 2015 Aug;30(4):787-92. doi: 10.1016/j.jcrc.2015.03.017. Epub 2015 Mar 22. J Crit Care. 2015. PMID: 25964208 Clinical Trial.
-
Chlorhexidine, toothbrushing, and preventing ventilator-associated pneumonia in critically ill adults.Am J Crit Care. 2009 Sep;18(5):428-37; quiz 438. doi: 10.4037/ajcc2009792. Am J Crit Care. 2009. PMID: 19723863 Free PMC article. Clinical Trial.
-
Oral mucosal decontamination with chlorhexidine for the prevention of ventilator-associated pneumonia in children - a randomized, controlled trial.Pediatr Crit Care Med. 2012 Sep;13(5):e305-10. doi: 10.1097/PCC.0b013e31824ea119. Pediatr Crit Care Med. 2012. PMID: 22760426 Clinical Trial.
-
Oral Chlorhexidine Use to Prevent Ventilator-Associated Pneumonia in Adults: Review of the Current Literature.Dimens Crit Care Nurs. 2016 Jan-Feb;35(1):25-36. doi: 10.1097/DCC.0000000000000154. Dimens Crit Care Nurs. 2016. PMID: 26627070 Review.
-
Oropharyngeal Decontamination with Antiseptics to Prevent Ventilator-Associated Pneumonia: Rethinking the Benefits of Chlorhexidine.Semin Respir Crit Care Med. 2017 Jun;38(3):381-390. doi: 10.1055/s-0037-1602584. Epub 2017 Jun 4. Semin Respir Crit Care Med. 2017. PMID: 28578560 Review.
Cited by
-
Implementation of an ED-based bundled mechanical ventilation protocol improves adherence to lung-protective ventilation.Am J Emerg Med. 2021 May;43:186-194. doi: 10.1016/j.ajem.2020.02.053. Epub 2020 Feb 25. Am J Emerg Med. 2021. PMID: 32139215 Free PMC article. No abstract available.
-
Efficacy of a bundle approach in preventing the incidence of ventilator associated pneumonia (VAP).Bosn J Basic Med Sci. 2018 Feb 20;18(1):105-109. doi: 10.17305/bjbms.2017.2278. Bosn J Basic Med Sci. 2018. PMID: 28976870 Free PMC article.
References
-
- Eom JS, Lee MS, Chun HK, et al. The impact of a ventilator bundle on preventing ventilator-associated pneumonia: a multicenter study. American journal of infection control. 2014;42(1):34–37. - PubMed
-
- To KB, Napolitano LM. Common complications in the critically ill patient. The Surgical clinics of North America. 2012;92(6):1519–1557. - PubMed
-
- Cutler LR, Sluman P. Reducing ventilator associated pneumonia in adult patients through high standards of oral care: a historical control study. Intensive & critical care nursing : the official journal of the British Association of Critical Care Nurses. 2014;30(2):61–68. - PubMed
-
- Chan EY. Oral decontamination with chlorhexidine reduced ventilator associated pneumonia in patients needing mechanical ventilation for >/=48 hours. Evidence-based nursing. 2007;10(1):19. - PubMed
-
- Kollef MH. Ventilator-associated pneumonia. A multivariate analysis. JAMA : the journal of the American Medical Association. 1993;270(16):1965–1970. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
