

Impact of multimodal therapy in locally recurrent rectal cancer
- PMID: 26933792
- PMCID: PMC5407413
- DOI: 10.1002/bjs.10079
Impact of multimodal therapy in locally recurrent rectal cancer
Abstract
Background: The practice of salvaging recurrent rectal cancer has evolved. The aim of this study was to define the evolving salvage potential over time among patients with locally recurrent disease, and to identify durable determinants of long-term success.
Methods: The study included consecutive patients with recurrent rectal cancer undergoing multimodal salvage with curative intent between 1988 and 2012. Predictors of long-term survival were defined by Cox regression analysis and compared over time. Re-recurrence and subsequent treatments were evaluated.
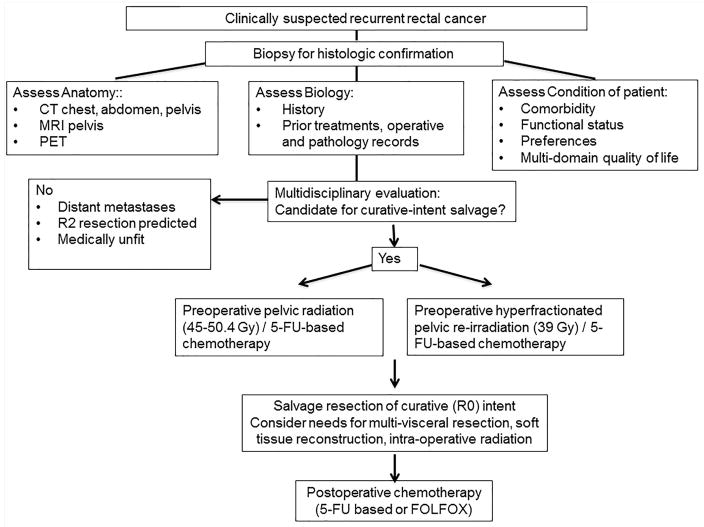
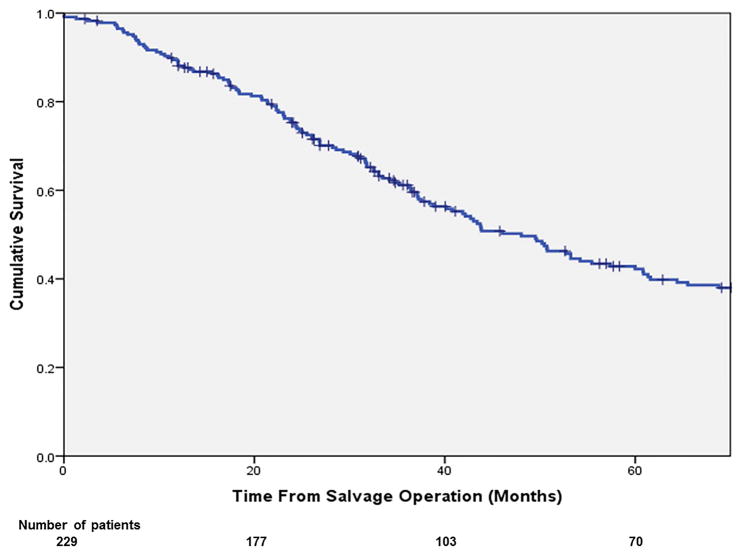
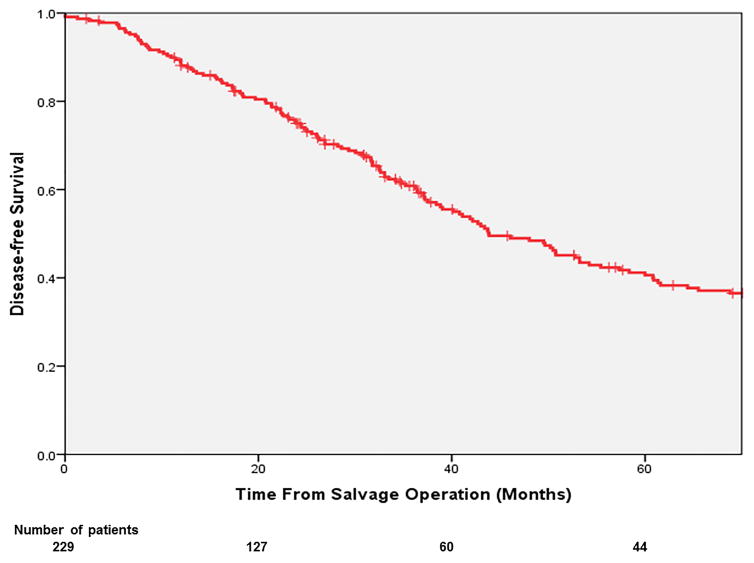
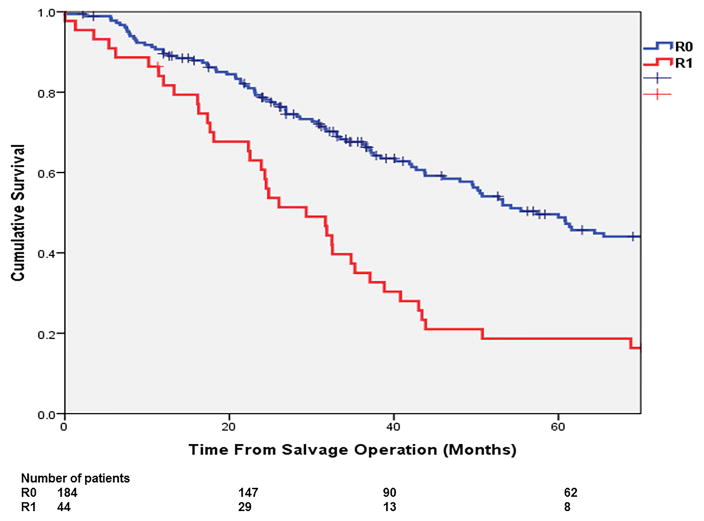
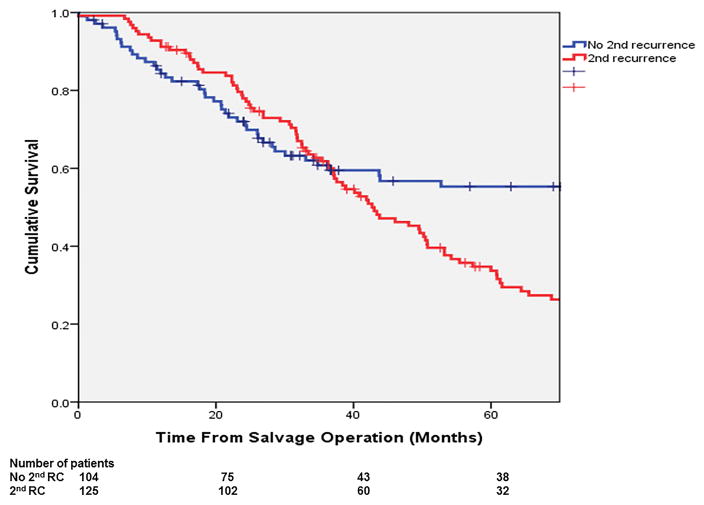
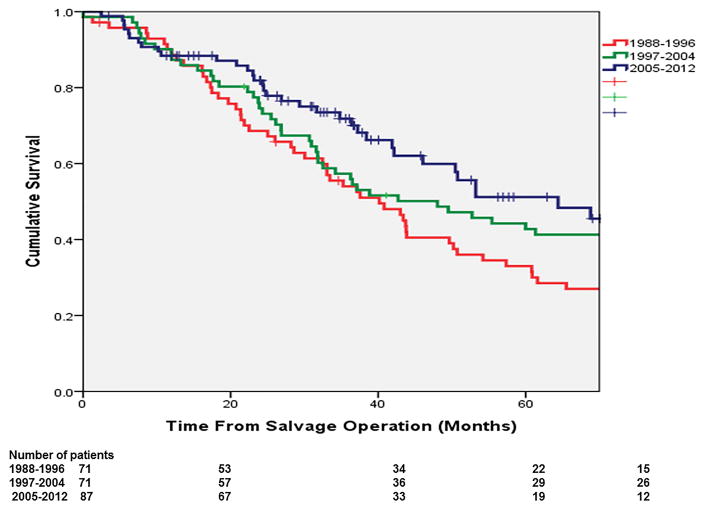
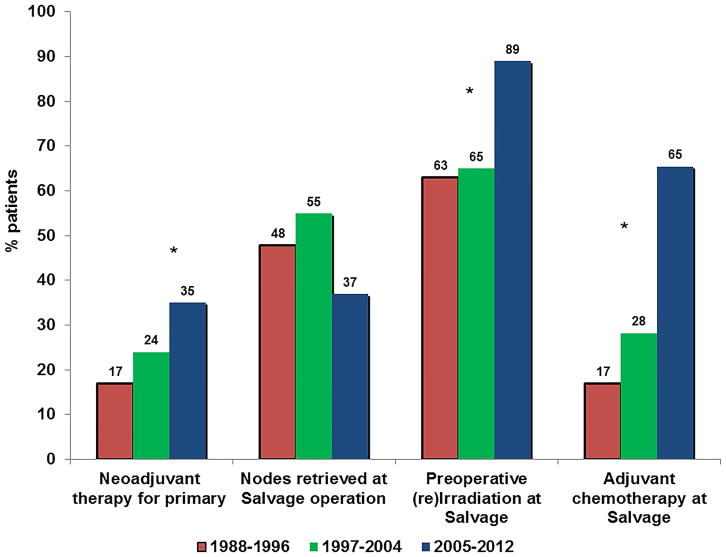
Results: After multidisciplinary evaluation of 229 patients, salvage therapy with curative intent included preoperative chemotherapy and/or radiotherapy (73·4 per cent; with 41·3 per cent undergoing repeat pelvic irradiation), surgical salvage resection with or without intraoperative irradiation (36·2 per cent), followed by postoperative adjuvant chemotherapy (38·0 per cent). Multivisceral resection was undertaken in 47·2 per cent and bone resection in 29·7 per cent. The R0 resection rate was 80·3 per cent. After a median follow-up of 56·5 months, the 5-year overall survival rate was 50 per cent in 2005-2012, markedly increased from 32 per cent in 1988-1996 (P = 0·044). Long-term success was associated with R0 resection (P = 0·017) and lack of secondary failure (P = 0·003). Some 125 patients (54·6 per cent) developed further recurrence at a median of 19·4 months after salvage surgery. Repeat operative rescue was feasible in 21 of 48 patients with local re-recurrence alone and in 17 of 77 with distant re-recurrence, with a median survival of 19·8 months after further recurrence.
Conclusion: The long-term salvage potential for recurrent rectal cancer improved significantly over time, with the introduction of an individualized treatment algorithm of multimodal treatments and surgical salvage. Durable predictors of long-term success were R0 resection at salvage operation, avoidance of secondary failure, and feasibility of repeat rescue after re-recurrence.
© 2016 BJS Society Ltd Published by John Wiley & Sons Ltd.
Figures
References
-
- Rodriguez-Bigas MA, Chang GJ, Skibber JM. Multidisciplinary approach to recurrent/unresectable rectal cancer: how to prepare for the extent of resection. Surg Oncol Clin N Am. 2010;19(4):847–859. - PubMed
-
- Sauer R, Becker H, Hohenberger W, Rodel C, Wittekind C, Fietkau R, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. The New England journal of medicine. 2004;351(17):1731–1740. - PubMed
-
- Kapiteijn E, Marijnen CA, Nagtegaal ID, Putter H, Steup WH, Wiggers T, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. The New England journal of medicine. 2001;345(9):638–646. - PubMed
-
- Park IJ, You YN, Agarwal A, Skibber JM, Rodriguez-Bigas MA, Eng C, et al. Neoadjuvant treatment response as an early response indicator for patients with rectal cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2012;30(15):1770–1776. - PMC - PubMed
-
- Sauer R, Liersch T, Merkel S, Fietkau R, Hohenberger W, Hess C, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2012;30(16):1926–1933. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
