

Association of Red Blood Cell Transfusion, Anemia, and Necrotizing Enterocolitis in Very Low-Birth-Weight Infants
- PMID: 26934258
- PMCID: PMC4805423
- DOI: 10.1001/jama.2016.1204
Association of Red Blood Cell Transfusion, Anemia, and Necrotizing Enterocolitis in Very Low-Birth-Weight Infants
Abstract
Importance: Data regarding the contribution of red blood cell (RBC) transfusion and anemia to necrotizing enterocolitis (NEC) are conflicting. These associations have not been prospectively evaluated, accounting for repeated, time-varying exposures.
Objective: To determine the relationship between RBC transfusion, severe anemia, and NEC.
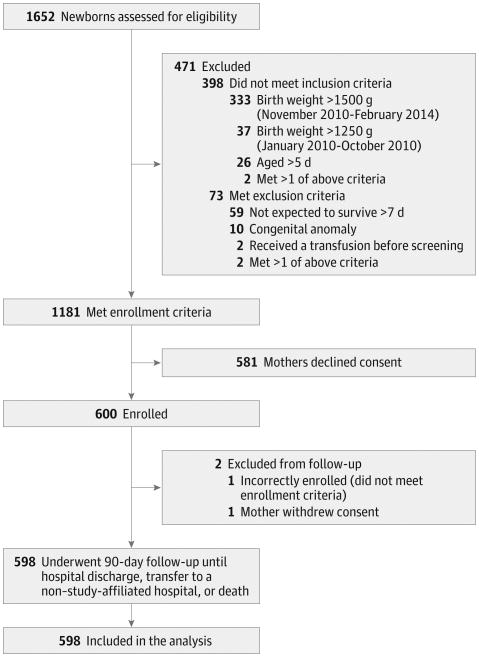
Design, setting, and participants: In a secondary, prospective, multicenter observational cohort study from January 2010 to February 2014, very low-birth-weight (VLBW, ≤1500 g) infants, within 5 days of birth, were enrolled at 3 level III neonatal intensive care units in Atlanta, Georgia. Two hospitals were academically affiliated and 1 was a community hospital. Infants received follow-up until 90 days, hospital discharge, transfer to a non-study-affiliated hospital, or death (whichever came first). Multivariable competing-risks Cox regression was used, including adjustment for birth weight, center, breastfeeding, illness severity, and duration of initial antibiotic treatment, to evaluate the association between RBC transfusion, severe anemia, and NEC.
Exposures: The primary exposure was RBC transfusion. The secondary exposure was severe anemia, defined a priori as a hemoglobin level of 8 g/dL or less. Both exposures were evaluated as time-varying covariates at weekly intervals.
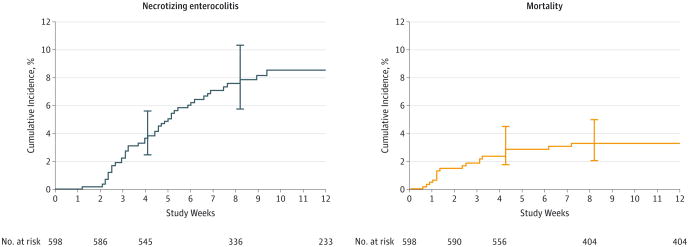
Main outcomes and measures: Necrotizing enterocolitis, defined as Bell stage 2 or greater by preplanned adjudication. Mortality was evaluated as a competing risk.
Results: Of 600 VLBW infants enrolled, 598 were evaluated. Forty-four (7.4%) infants developed NEC. Thirty-two (5.4%) infants died (all cause). Fifty-three percent of infants (319) received a total of 1430 RBC transfusion exposures. The unadjusted cumulative incidence of NEC at week 8 among RBC transfusion-exposed infants was 9.9% (95% CI, 6.9%-14.2%) vs 4.6% (95% CI, 2.6%-8.0%) among those who were unexposed. In multivariable analysis, RBC transfusion in a given week was not significantly related to the rate of NEC (adjusted cause-specific hazard ratio, 0.44 [95% CI, 0.17-1.12]; P = .09). Based on evaluation of 4565 longitudinal measurements of hemoglobin (median, 7 per infant), the rate of NEC was significantly increased among VLBW infants with severe anemia in a given week compared with those who did not have severe anemia (adjusted cause-specific hazard ratio, 5.99 [95% CI, 2.00-18.0]; P = .001).
Conclusions and relevance: Among VLBW infants, severe anemia, but not RBC transfusion, was associated with an increased risk of NEC. Further studies are needed to evaluate whether preventing severe anemia is more important than minimizing RBC transfusion.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
