

Prevalence of Combined Somatic and Mental Health Multimorbidity: Patterns by Age, Sex, and Race/Ethnicity
- PMID: 26935110
- PMCID: PMC5055644
- DOI: 10.1093/gerona/glw032
Prevalence of Combined Somatic and Mental Health Multimorbidity: Patterns by Age, Sex, and Race/Ethnicity
Abstract
Background: The coexistence of chronic mental health conditions with somatic conditions (somatic-mental multimorbidity, or SMM) is common and has been associated with greater symptom burden and functional impairment, higher costs, and excess mortality. However, most existing literature focused on the co-occurrence of an index mental health condition with specific additional conditions. By contrast, we studied the prevalence and patterns of SMM more broadly considering 19 selected conditions, and we focused on differences by age, sex, and race/ethnicity.
Methods: The Rochester Epidemiology Project (REP) records-linkage system was used to identify all residents of Olmsted County, MN, on April 1, 2010. We identified individuals with each of 19 common chronic conditions, including 5 mental health conditions, using the International Classification of Diseases, ninth revision (ICD-9) codes received from any health care provider between April 1, 2005 and March 31, 2010.
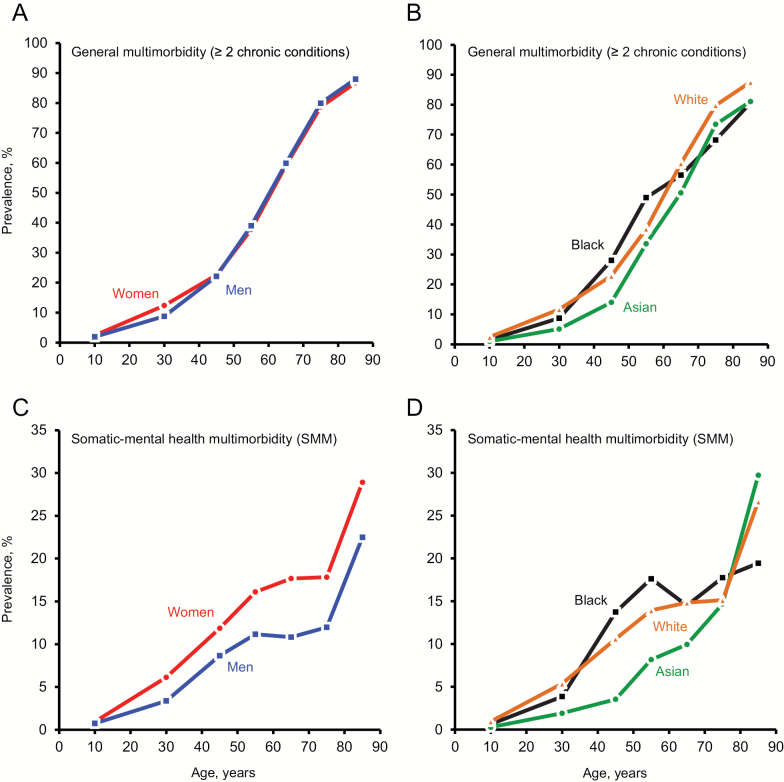
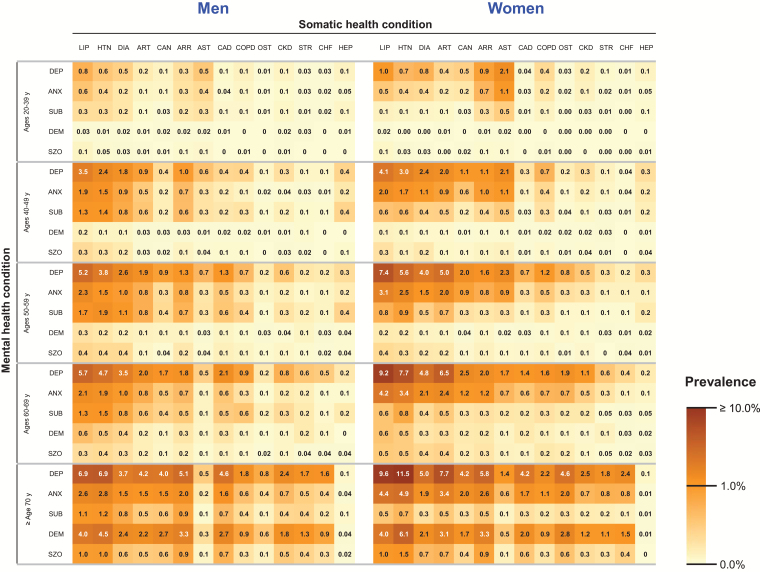
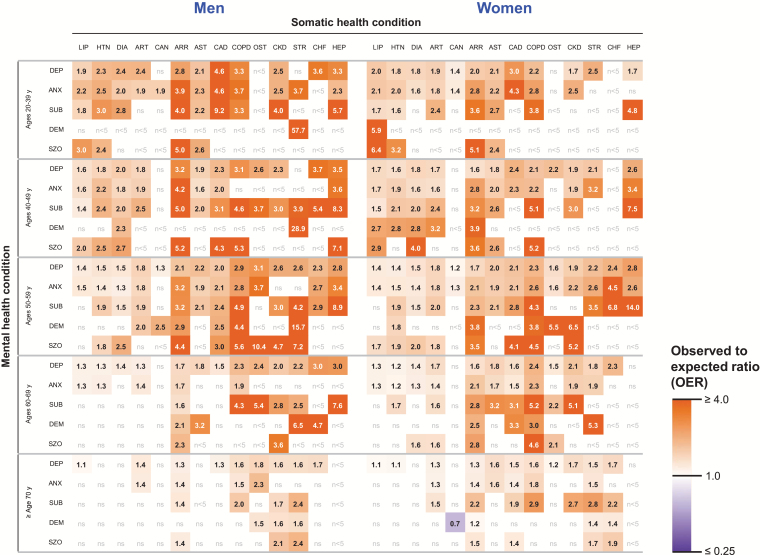
Results: Among the 138,858 residents of the county, 52.4% were women, and 7.9% had SMM. SMM increased steeply with older age, was 1.7 times more common in women, and was lower in Asians compared with whites. Of the 10,903 persons with SMM, 7,739 (71.0%) were younger than 65 years. Depressive and anxiety disorders were the most common conditions involved in SMM. The dyads that were observed more frequently or less frequently than expected by chance varied in composition by age and sex.
Conclusions: SMM that reaches medical attention is highly prevalent across all age groups, is more frequent in women, is less frequent in Asians, and encompasses a wide range of conditions.
Keywords: Age; Mental health multimorbidity; Race/ethnicity; Sex; Somatic multimorbidity.
© The Author 2016. Published by Oxford University Press on behalf of The Gerontological Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Hoffman C, Rice D, Sung HY. Persons with chronic conditions. Their prevalence and costs. JAMA. 1996;276:1473–1479. doi:10.1001/jama.1996.03540180029029 - PubMed
-
- Kronick R, Bella M, Gilmer T. The Faces of Medicaid III: Refining the Portrait of People With Multiple Chronic Conditions. Hamilton, NJ: Center for Health Care Strategies, Inc; 2009.
-
- Neeleman J, Ormel J, Bijl RV. The distribution of psychiatric and somatic III health: associations with personality and socioeconomic status. Psychosom Med. 2001;63:239–247. - PubMed
-
- Viron MJ, Stern TA. The impact of serious mental illness on health and healthcare. Psychosomatics. 2010;51:458–465. doi:10.1176/appi.psy.51.6.458 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
