

Lay support for pregnant women with social risk: a randomised controlled trial
- PMID: 26936901
- PMCID: PMC4785315
- DOI: 10.1136/bmjopen-2015-009203
Lay support for pregnant women with social risk: a randomised controlled trial
Abstract
Objectives: We sought evidence of effectiveness of lay support to improve maternal and child outcomes in disadvantaged families.
Design: Prospective, pragmatic, individually randomised controlled trial.
Setting: 3 Maternity Trusts in West Midlands, UK.
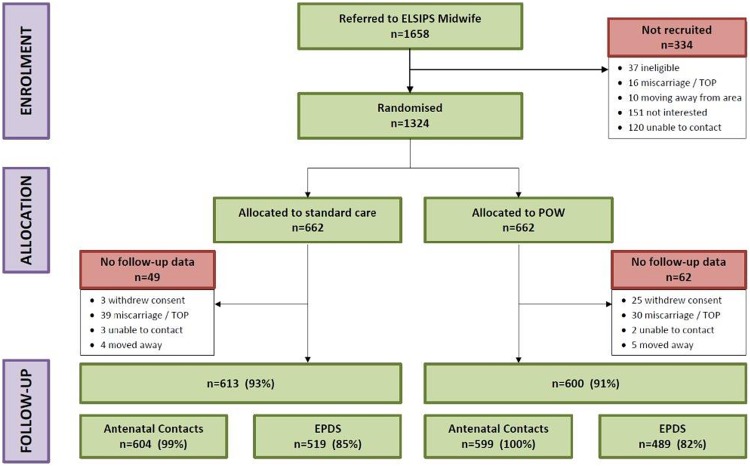
Participants: Following routine midwife systematic assessment of social risk factors, 1324 nulliparous women were assigned, using telephone randomisation, to standard maternity care, or addition of referral to a Pregnancy Outreach Worker (POW) service. Those under 16 years and teenagers recruited to the Family Nurse Partnership trial were excluded.
Interventions: POWs were trained to provide individual support and case management for the women including home visiting from randomisation to 6 weeks after birth. Standard maternity care (control) included provision for referring women with social risk factors to specialist midwifery services, available to both arms.
Main outcome measures: Primary outcomes were antenatal visits attended and Edinburgh Postnatal Depression Scale (EPDS) 8-12 weeks postpartum. Prespecified, powered, subgroup comparison was among women with 2 or more social risks. Secondary outcomes included maternal and neonatal birth outcomes; maternal self-efficacy, and mother-to-infant bonding at 8-12 weeks; child development assessment at 6 weeks, breastfeeding at 6 weeks, and immunisation uptake at 4 months, all collected from routine child health systems.
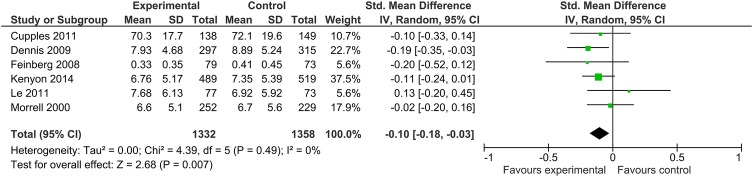
Results: Antenatal attendances were high in the standard care control and did not increase further with addition of the POW intervention (10.1 vs 10.1 (mean difference; MD) -0.00, 95% CI (95% CI -0.37 to 0.37)). In the powered subgroup of women with 2 or more social risk factors, mean EPDS (MD -0.79 (95% CI -1.56 to -0.02) was significantly better, although for all women recruited, no significant differences were seen (MD -0.59 (95% CI -1.24 to 0.06). Mother-to-infant bonding was significantly better in the intervention group for all women (MD -0.30 (95% CI -0.61 to -0.00) p=0.05), and there were no differences in other secondary outcomes.
Conclusions: This trial demonstrates differences in depressive symptomatology with addition of the POW service in the powered subgroup of women with 2 or more social risk factors. Addition to existing evidence indicates benefit from lay interventions in preventing postnatal depression. This finding is important for women and their families given the known effect of maternal depression on longer term childhood outcomes.
Trial registration number: ISRCTN35027323; Results.
Keywords: OBSTETRICS; PUBLIC HEALTH; pregnancy; social/lay support.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
-
- O'Hara M, Swain A. Rates and risk of postpartum depression—a meta–analysis. Int Rev Psychiatry 1996;8:37–54. 10.3109/09540269609037816 - DOI
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical