

How effective is an in-hospital heart failure self-care program in a Japanese setting? Lessons from a randomized controlled pilot study
- PMID: 26937177
- PMCID: PMC4762442
- DOI: 10.2147/PPA.S100203
How effective is an in-hospital heart failure self-care program in a Japanese setting? Lessons from a randomized controlled pilot study
Abstract
Background: Although the effectiveness of heart failure (HF) disease management programs has been established in Western countries, to date there have been no such programs in Japan. These programs may have different effectiveness due to differences in health care organization and possible cultural differences with regard to self-care. Therefore, the purpose of this study was to evaluate the effectiveness of a pilot HF program in a Japanese setting.
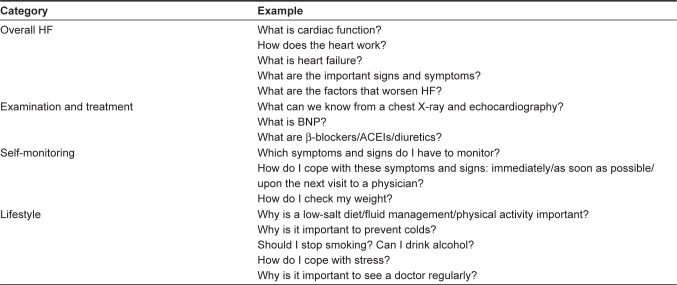
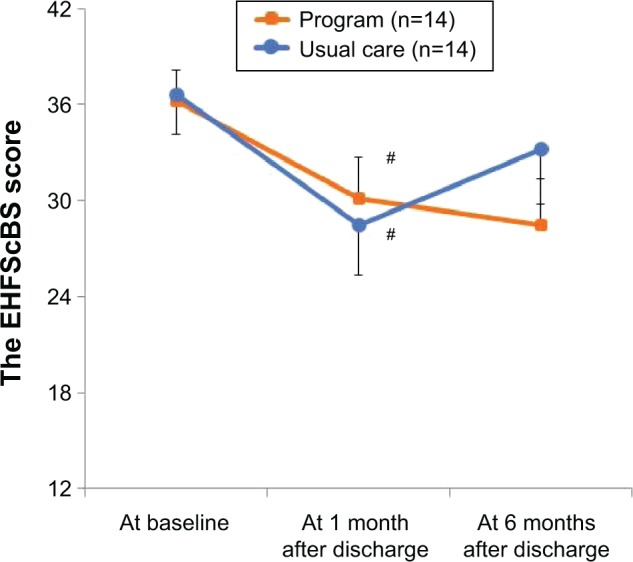
Methods: We developed an HF program focused on enhancing patient self-care before hospital discharge. Patients were randomized 1:1 to receive the new HF program or usual care. The primary outcome was self-care behavior as assessed by the European Heart Failure Self-Care Behavior Scale (EHFScBS). Secondary outcomes included HF knowledge and the 2-year rate of HF hospitalization and/or cardiac death.
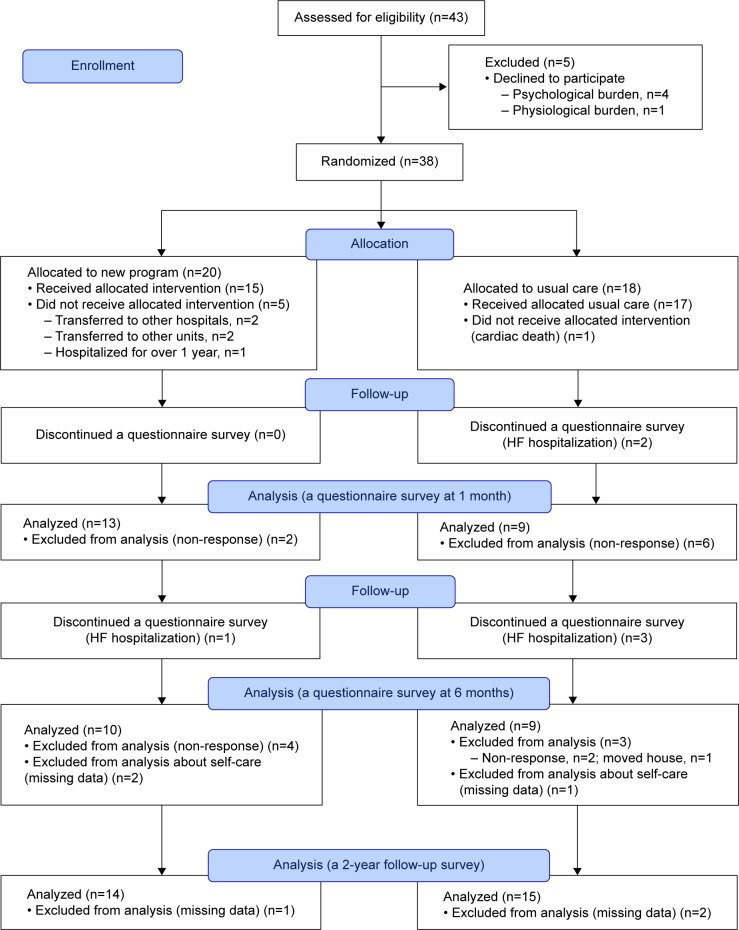
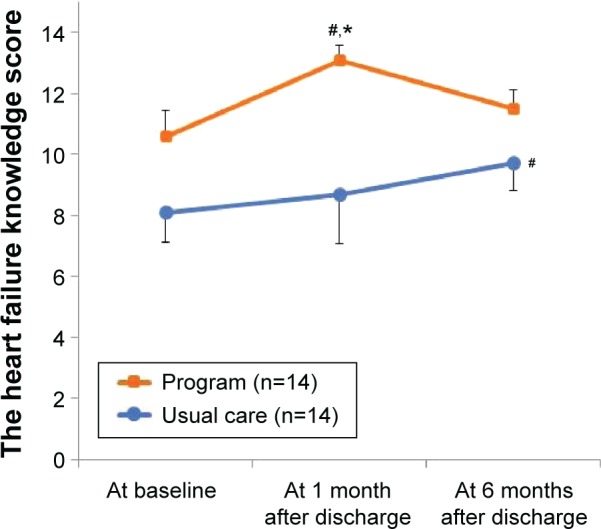
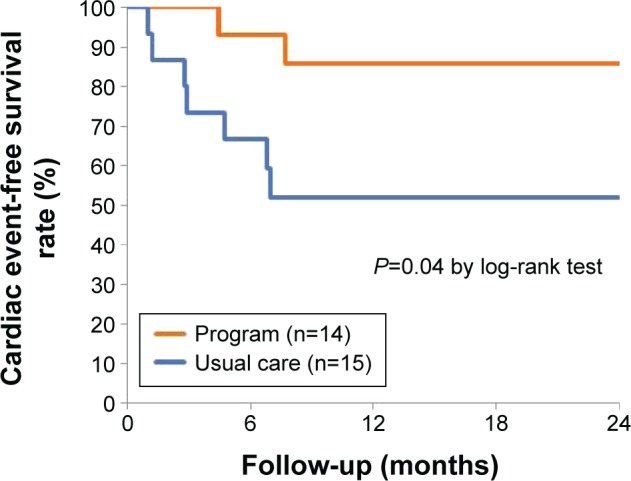
Results: A total of 32 patients were enrolled (mean age, 63 years; 31% female). There was no difference in the total score of the EHFScBS between the two groups. One specific behavior score regarding a low-salt diet significantly improved compared with baseline in the intervention group. HF knowledge in the intervention group tended to improve more over 6 months than in the control group (a group-by-time effect, F=2.47, P=0.098). During a 2-year follow-up, the HF program was related to better outcomes regarding HF hospitalization and/or cardiac death (14% vs 48%, log-rank test P=0.04). In Cox regression analysis after adjustment for age, sex, and logarithmic of B-type natriuretic peptide, the program was associated with a reduction in HF hospitalization and/or cardiac death (hazard ratio, 0.17; 95% confidence interval, 0.03-0.90; P=0.04).
Conclusion: The HF program was likely to increase patients' HF knowledge, change their behavior regarding a low-salt diet, and reduce HF hospitalization and/or cardiac events. Further improvement focused on the transition of knowledge to self-care behavior is necessary.
Keywords: discharge education; disease management; hospitalization; knowledge; nursing; patient education.
Figures
References
-
- Okura Y, Ramadan MM, Ohno Y, et al. Impending epidemic: future projection of heart failure in Japan to the year 2055. Circ J. 2008;72(3):489–491. - PubMed
-
- Riegel B, Moser DK, Anker SD, et al. State of the science: promoting self-care in persons with heart failure: a scientific statement from the American Heart Association. Circulation. 2009;120(12):1141–1163. - PubMed
-
- Jaarsma T, Stromberg A. Heart failure clinics are still useful (more than ever?) Can J Cardiol. 2014;30(3):272–275. - PubMed
-
- McAlister FA, Stewart S, Ferrua S, McMurray JJJV. Multidisciplinary strategies for the management of heart failure patients at high risk for admission: a systematic review of randomized trials. J Am Coll Cardiol. 2004;44(4):810–819. - PubMed
-
- Wakefield BJ, Boren SA, Groves PS, Conn VS. Heart failure care management programs: a review of study interventions and meta-analysis of outcomes. J Cardiovasc Nurs. 2013;28(1):8–19. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
