

Diagnosis, assessment, and phenotyping of COPD: beyond FEV₁
- PMID: 26937185
- PMCID: PMC4765947
- DOI: 10.2147/COPD.S85976
Diagnosis, assessment, and phenotyping of COPD: beyond FEV₁
Abstract
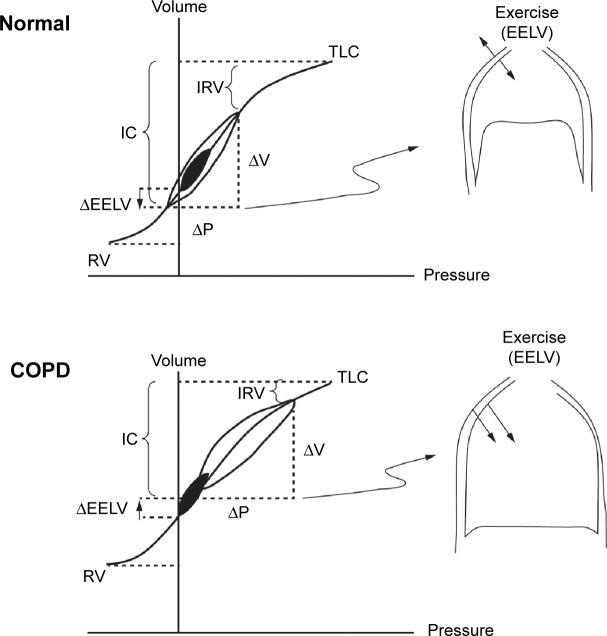
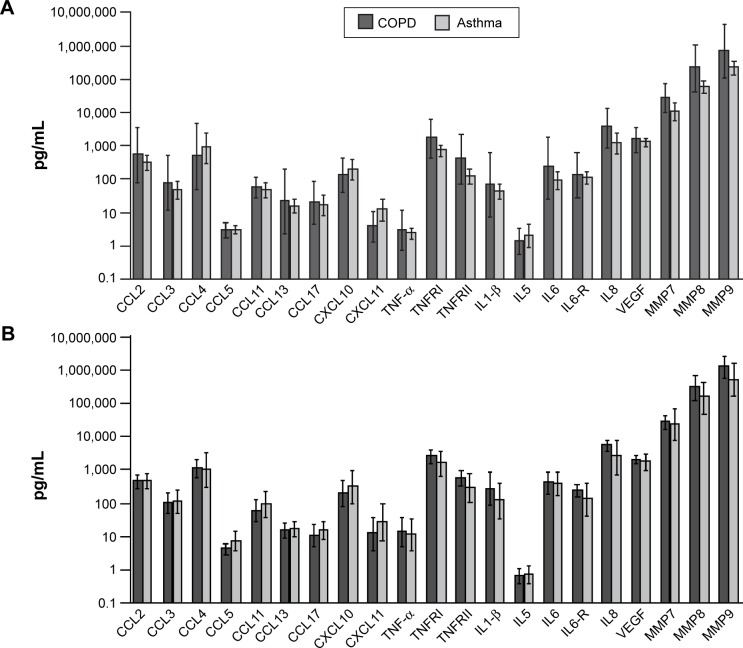
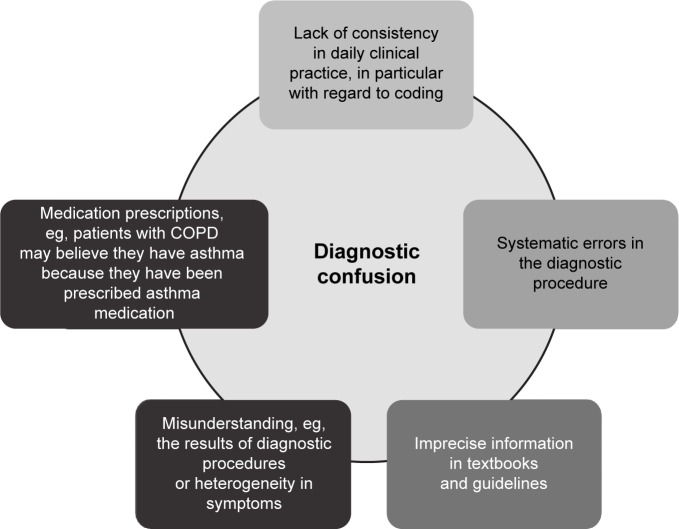
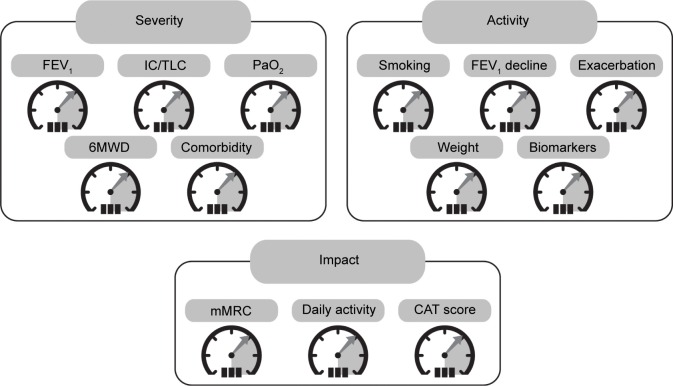
COPD is now widely recognized as a complex heterogeneous syndrome, having both pulmonary and extrapulmonary features. In clinical practice, the diagnosis of COPD is based on the presence of chronic airflow limitation, as assessed by post-bronchodilator spirometry. The severity of the airflow limitation, as measured by percent predicted FEV1, provides important information to the physician to enable optimization of management. However, in order to accurately assess the complexity of COPD, there need to be other measures made beyond FEV1. At present, there is a lack of reliable and simple blood biomarkers to confirm and further assess the diagnosis of COPD. However, it is possible to identify patients who display different phenotypic characteristics of COPD that relate to clinically relevant outcomes. Currently, validated phenotypes of COPD include alpha-1 antitrypsin deficiency, and "frequent exacerbators". Recently, a definition and assessment of a new phenotype comprising patients with overlapping features of asthma and COPD has been suggested and is known as "asthma COPD overlap syndrome". Several other phenotypes have been proposed, but require validation against clinical outcomes. Defining phenotypes requires the assessment of multiple factors indicating disease severity, its impact, and its activity. Recognition and validation of COPD phenotypes has an important role to play in the selection of evidence-based targeted therapy in the future management of COPD, but regardless of the diagnostic terms, patients with COPD should be assessed and treated according to their individual treatable characteristics.
Keywords: ACOS; COPD; asthma; diagnosis; phenotype.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease [updated 2015] [Accessed March 30, 2015]. Available from: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2015_Feb18.pdf.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
