

Exacerbations of COPD
- PMID: 26937187
- PMCID: PMC4764047
- DOI: 10.2147/COPD.S85978
Exacerbations of COPD
Abstract
Exacerbations of chronic obstructive pulmonary disease (COPD) are defined as sustained worsening of a patient's condition beyond normal day-to-day variations that is acute in onset, and that may also require a change in medication and/or hospitalization. Exacerbations have a significant and prolonged impact on health status and outcomes, and negative effects on pulmonary function. A significant proportion of exacerbations are unreported and therefore left untreated, leading to a poorer prognosis than those treated. COPD exacerbations are heterogeneous, and various phenotypes have been proposed which differ in biologic basis, prognosis, and response to therapy. Identification of biomarkers could enable phenotype-driven approaches for the management and prevention of exacerbations. For example, several biomarkers of inflammation can help to identify exacerbations most likely to respond to oral corticosteroids and antibiotics, and patients with a frequent exacerbator phenotype, for whom preventative treatment is appropriate. Reducing the frequency of exacerbations would have a beneficial impact on patient outcomes and prognosis. Preventative strategies include modification of risk factors, treatment of comorbid conditions, the use of bronchodilator therapy with long-acting β2-agonists or long-acting muscarinic antagonists, and inhaled corticosteroids. A better understanding of the mechanisms underlying COPD exacerbations will help to optimize use of the currently available and new interventions for preventing and treating exacerbations.
Keywords: COPD; biomarker; bronchodilator; exacerbation; phenotype.
Figures
References
-
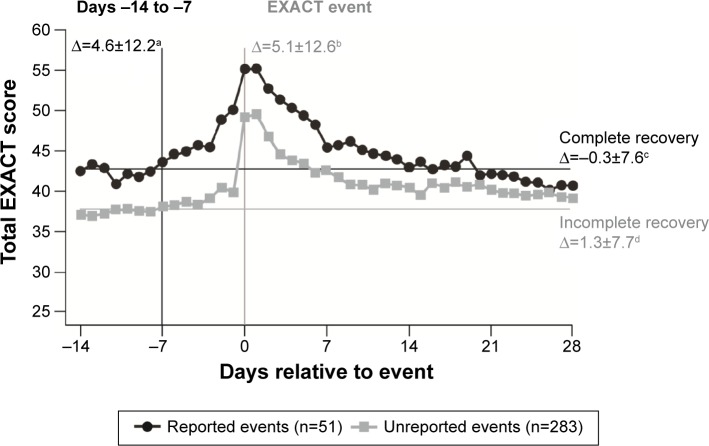
- Jones PW, Lamarca R, Chuecos F, et al. Characterisation and impact of reported and unreported exacerbations: results from ATTAIN. Eur Respir J. 2014;44(5):1156–1165. - PubMed
-
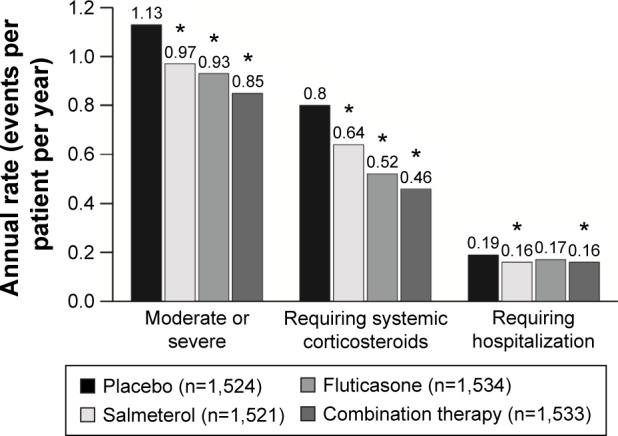
- Celli BR, Thomas NE, Anderson JA, et al. Effect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: results from the TORCH study. Am J Respir Crit Care Med. 2008;178(4):332–338. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
