

Early Diagnosis of Pneumonia in Severe Stroke: Clinical Features and the Diagnostic Role of C-Reactive Protein
- PMID: 26937636
- PMCID: PMC4777448
- DOI: 10.1371/journal.pone.0150269
Early Diagnosis of Pneumonia in Severe Stroke: Clinical Features and the Diagnostic Role of C-Reactive Protein
Abstract
Background: Accurate diagnosis of pneumonia complicating severe stroke is challenging due to difficulties in physical examination, altered immune responses and delayed manifestations of radiological changes. The aims of this study were to describe early clinical features and to examine C-reactive protein (CRP) as a diagnostic marker of post-stroke pneumonia.
Methods: Patients who required nasogastric feeding and had no evidence of pneumonia within 7 days of stroke onset were included in the study and followed-up for 21 days with a daily clinical examination. Pneumonia was diagnosed using modified British Thoracic Society criteria.
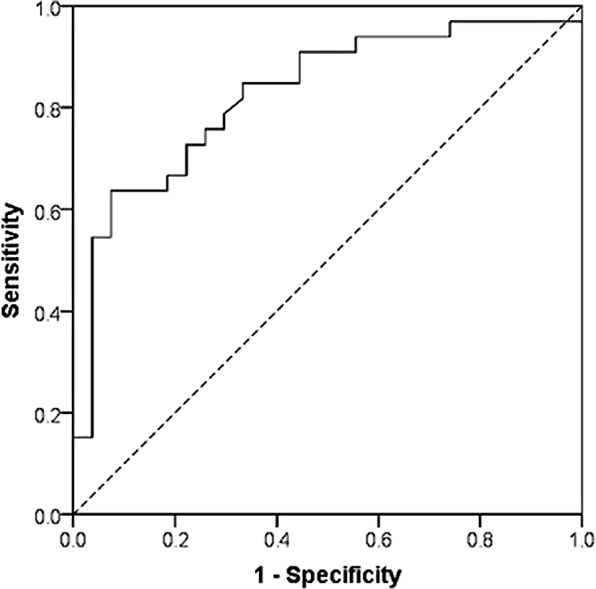
Results: 60 patients were recruited (mean age 77 years, mean National Institutes of Health Stroke Scale Score 19.47). Forty-four episodes of pneumonia were identified. Common manifestations on the day of the diagnosis were new onset crackles (43/44, 98%), tachypnoea>25/min (42/44, 95%), and oxygen saturation <90% (41/44, 93%). Cough, purulent sputum, and pyrexia >38°C were observed in 27 (61%), 25 (57%) and 15 (34%) episodes respectively. Leucocytosis (WBC>11,000/ml) and raised CRP (>10 mg/l) were observed in 38 (86%) and 43 (97%) cases of pneumonia respectively. The area under the ROC curve for CRP was 0.827 (95% CI 0.720, 0.933). The diagnostic cut-off for CRP with an acceptable sensitivity (>0.8) was 25.60 mg/L (Youden index (J) 0.515; sensitivity 0.848; specificity 0.667). A cut-off of 64.65 mg/L had the highest diagnostic accuracy (J 0.562; sensitivity 0.636; specificity 0.926).
Conclusion: Patients with severe stroke frequently do not manifest key diagnostic features of pneumonia such as pyrexia, cough and purulent sputum early in their illness. The most common signs in this group are new-onset crackles, tachypnoea and hypoxia. Our results suggest that a CRP >25 mg/L should prompt investigations for pneumonia while values >65 mg/L have the highest diagnostic accuracy to justify consideration of this threshold as a diagnostic marker of post-stroke pneumonia.
Conflict of interest statement
Figures
References
-
- Dirnagl U, Klehmet J, Braun JS, Harms H, Meisel C, Ziemssen T, et al. Stroke-induced immunodepression: experimental evidence and clinical relevance. Stroke 2007;38:770–773. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
