

Description and Validation of Histological Patterns and Proposal of a Dynamic Model of Inflammatory Infiltration in Giant-cell Arteritis
- PMID: 26937893
- PMCID: PMC4778989
- DOI: 10.1097/MD.0000000000002368
Description and Validation of Histological Patterns and Proposal of a Dynamic Model of Inflammatory Infiltration in Giant-cell Arteritis
Abstract
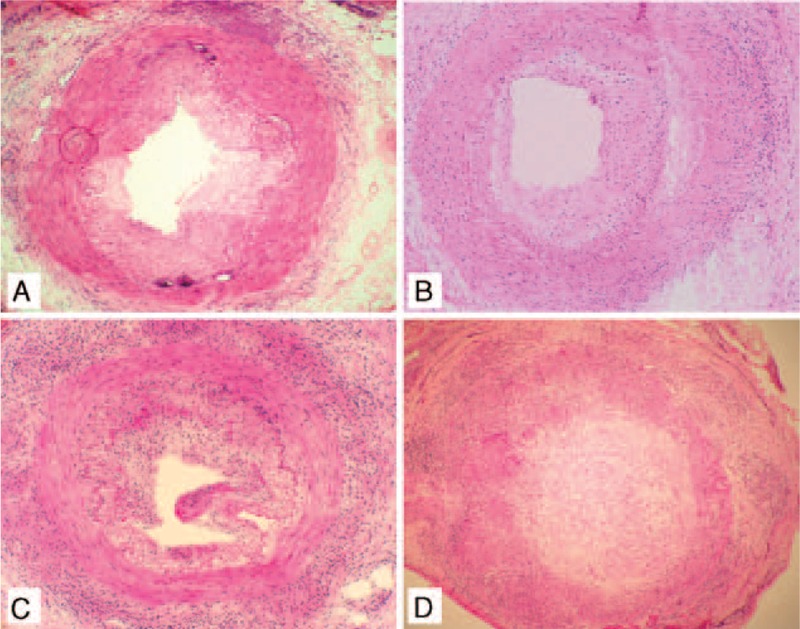
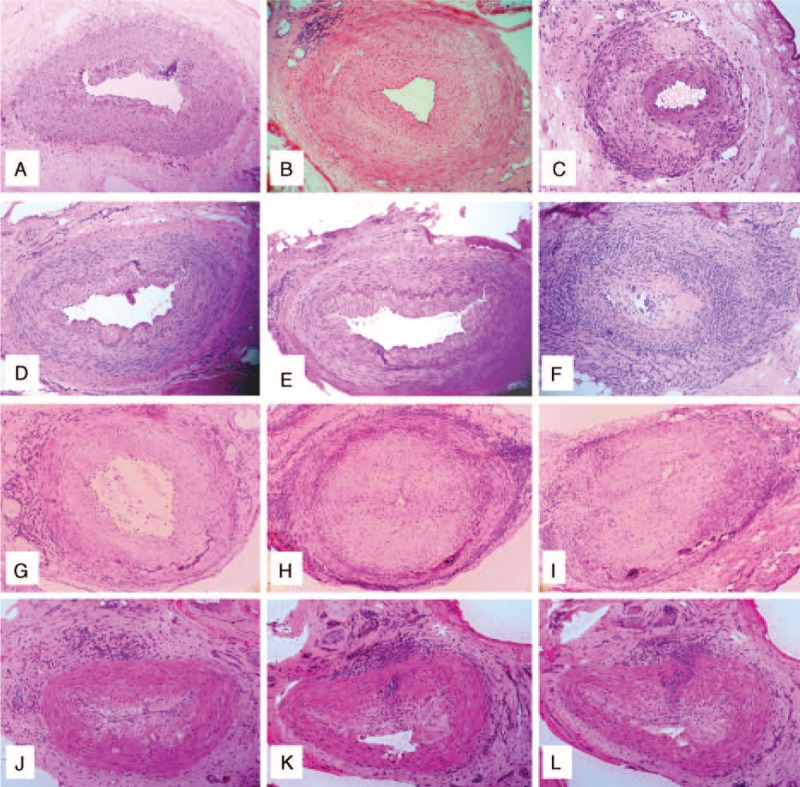
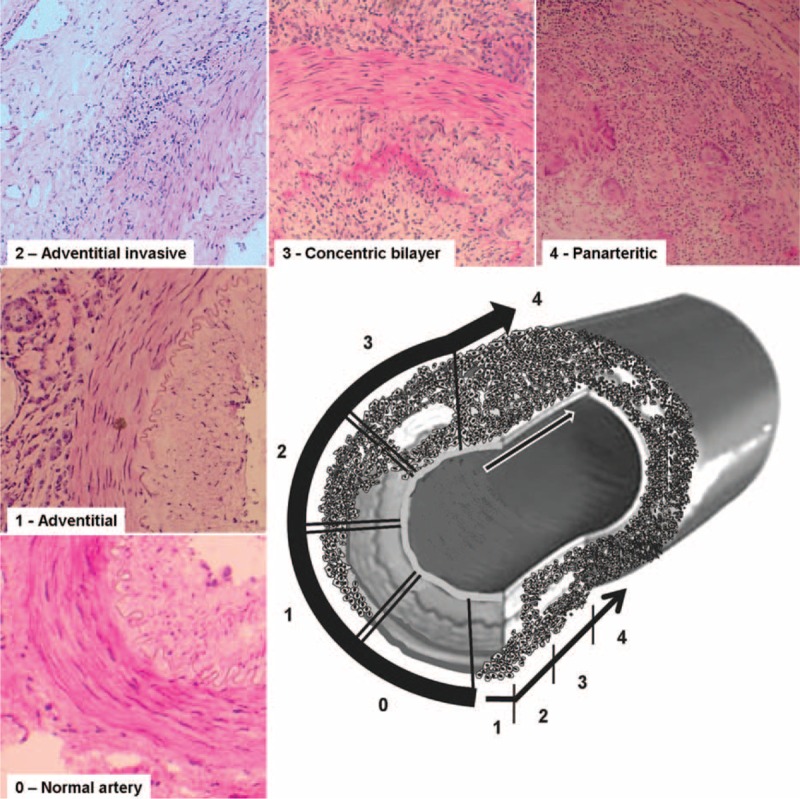
The extent of inflammatory infiltrates in arteries from patients with giant-cell arteritis (GCA) have been described using different terms and definitions. Studies investigating the relationship between GCA histological features and clinical manifestations have produced controversial results. The aims of this study were to characterize and validate histological patterns in temporal artery biopsies (TABs) from GCA patients, to explore additional histological features, including the coexistence of different patterns, and also to investigate the relationship of the inflammatory patterns with clinical and laboratory features.We performed histological examination of TAB from patients with GCA consecutively diagnosed between 1992 and 2012. Patterns of inflammation were defined according to the extent and distribution of inflammatory infiltrates within the artery. Clinical and laboratory variables were recorded. Two external investigators underwent a focused, one-day training session and then independently scored 77 cases. Quadratic-weighted kappa was calculated.TAB from 285 patients (200 female/85 male) were evaluated. Four histological inflammatory patterns were distinguished: 1 - adventitial (n = 16); 2 - adventitial invasive: adventitial involvement with some extension to the muscular layer (n = 21); 3 - concentric bilayer: adventitial and intimal involvement with media layer preservation (n = 52); and 4 - panarteritic (n = 196). Skip lesions were observed in 10% and coexistence of various patterns in 43%. Raw agreement of each external scorer with the gold-standard was 82% and 77% (55% and 46% agreement expected from chance); kappa = 0.82 (95% confidence interval [CI] 0.70-0.95) and 0.79 (95% CI 0.68-0.91). Although abnormalities on temporal artery palpation and the presence of jaw claudication and scalp tenderness tended to occur more frequently in patients with arteries depicting more extensive inflammation, no statistically significant correlations were found between histological patterns and clinical features or laboratory findings.In conclusion, we have described and validated 4 histological patterns. The presence of different coexisting patterns likely reflects sequential steps in the progression of inflammation and injury. No clear relationship was found between these patterns and clinical or laboratory findings. However, several cranial manifestations tended to occur more often in patients with temporal arteries exhibiting panarteritic inflammation. This validated score system may be useful to standardize stratification of histological severity for immunopathology biomarker studies or correlation with imaging.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Salvarani C, Cantini F, Hunder GG. Polymyalgia rheumatica and giant-cell arteritis. Lancet 2008; 372:234–245. - PubMed
-
- Cid MC, Font C, Coll-Vinent B, et al. Large vessel vasculitides. Curr Opin Rheumatol 1998; 10:18–28. - PubMed
-
- Cid MC, Campo E, Ercilla G, et al. Immunohistochemical analysis of lymphoid and macrophage cell subsets and their immunologic activation markers in temporal arteritis. Influence of corticosteroid treatment. Arthritis Rheum 1989; 32:884–893. - PubMed
-
- Lie JT. Temporal artery biopsy diagnosis of giant cell arteritis: lessons from 1109 biopsies. Anat Pathol 1996; 1:69–97. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
