

Predictors of Mortality Poorly Predict Common Measures of Disease Progression in Idiopathic Pulmonary Fibrosis
- PMID: 26938706
- PMCID: PMC5027229
- DOI: 10.1164/rccm.201508-1546OC
Predictors of Mortality Poorly Predict Common Measures of Disease Progression in Idiopathic Pulmonary Fibrosis
Abstract
Rationale: Mortality prediction is well studied in idiopathic pulmonary fibrosis (IPF), but little is known about predictors of premortality disease progression. Identification of patients at risk for disease progression would be useful for clinical decision-making and designing clinical trials.
Objectives: To develop prediction models for disease progression in IPF.
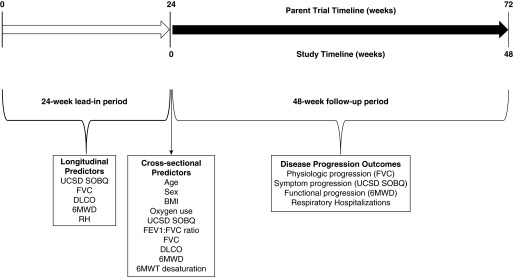
Methods: In a large clinical trial cohort of patients with IPF (n = 1,113), we comprehensively screened multivariate models of candidate baseline and past-change predictors for disease progression defined by 48-week worsening of FVC, dyspnea (University of California, San Diego Shortness of Breath Questionnaire [UCSD SOBQ]), 6-minute-walk distance (6MWD), and occurrence of respiratory hospitalization, or death. Progression outcomes were modeled as appropriate, by slope change using linear regression models and time to binary outcomes using Cox proportional hazards models.
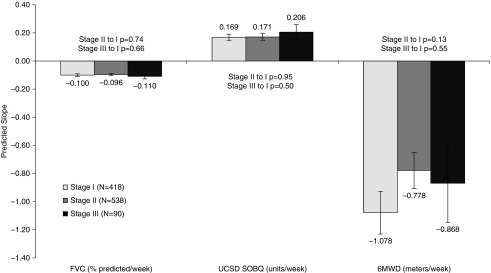
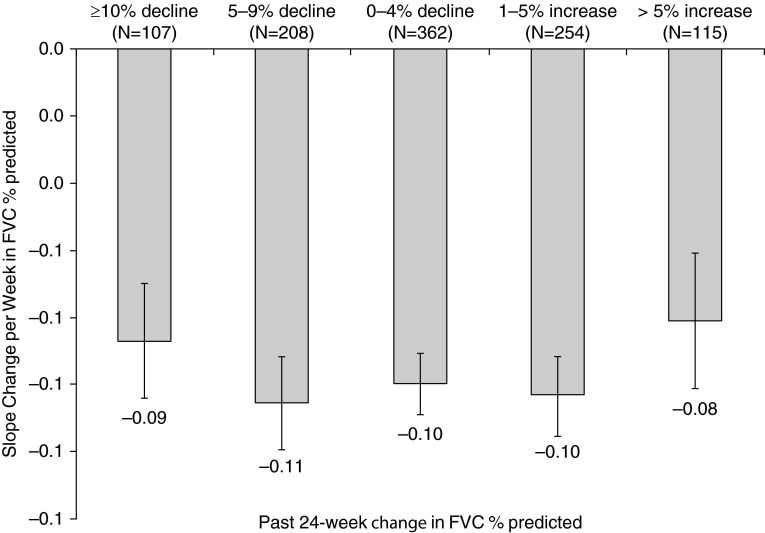
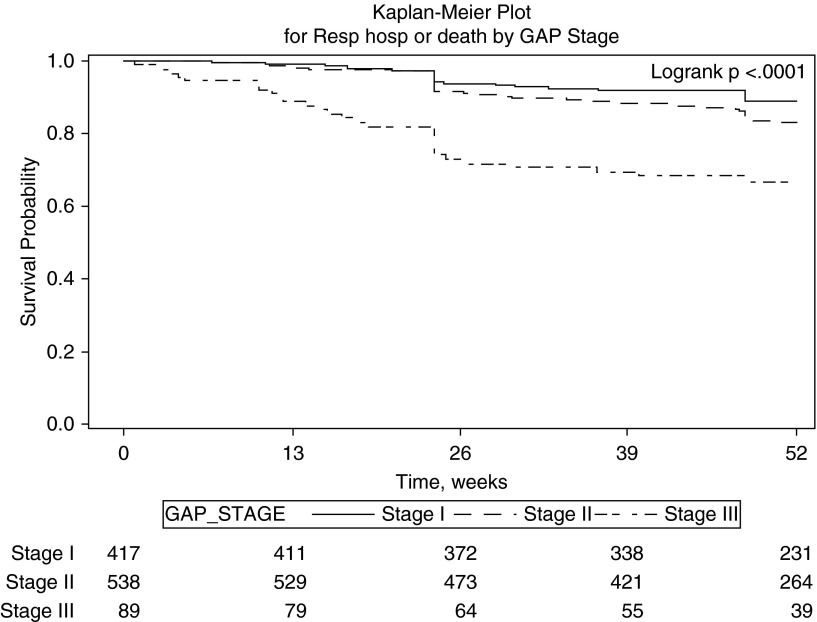
Measurements and main results: The overall cohort experienced considerable disease progression. Top-performing prediction models did not meaningfully predict most measures of disease progression. For example, prediction modeling explained less than or equal to 1% of the observed variation in 48-week slope change in FVC, UCSD SOBQ, and 6MWD. Models performed better for binary measures of time to disease progression but were still largely inaccurate (cross-validated C statistic ≤0.63 for ≥10% decline in FVC or death, ≤0.68 for ≥20-U increase in UCSD SOBQ or death, ≤0.70 for ≥100 m decline in 6MWD or death). Models for time to respiratory hospitalization or death (C statistic ≤0.77) or death alone (C statistic ≤0.81) demonstrated acceptable discriminative performance.
Conclusions: Clinical prediction models poorly predicted physiologic and functional disease progression in IPF. This is in contrast to respiratory hospitalization and mortality prediction.
Keywords: 6-minute-walk distance; dyspnea; forced vital capacity; hospitalization; interstitial lung disease.
Figures
Comment in
-
Clinical Trial Design Based on Time to Death/Progression.Am J Respir Crit Care Med. 2016 Sep 15;194(6):653-4. doi: 10.1164/rccm.201604-0819ED. Am J Respir Crit Care Med. 2016. PMID: 27628074 No abstract available.
References
-
- Raghu G, Collard HR, Egan JJ, Martinez FJ, Behr J, Brown KK, Colby TV, Cordier JF, Flaherty KR, Lasky JA, et al. ATS/ERS/JRS/ALAT Committee on Idiopathic Pulmonary Fibrosis. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183:788–824. - PMC - PubMed
-
- Ley B, Collard HR, King TE., Jr Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2011;183:431–440. - PubMed
-
- King TE, Jr, Bradford WZ, Castro-Bernardini S, Fagan EA, Glaspole I, Glassberg MK, Gorina E, Hopkins PM, Kardatzke D, Lancaster L, et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N Engl J Med. 2014;370:2083–2092. - PubMed
-
- Richeldi L, du Bois RM, Raghu G, Azuma A, Brown KK, Costabel U, Cottin V, Flaherty KR, Hansell DM, Inoue Y, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med. 2014;370:2071–2082. - PubMed
-
- Ley B, Ryerson CJ, Vittinghoff E, Ryu JH, Tomassetti S, Lee JS, Poletti V, Buccioli M, Elicker BM, Jones KD, et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann Intern Med. 2012;156:684–691. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
