

Incidence of AIDS-Defining Opportunistic Infections and Mortality during Antiretroviral Therapy in a Cohort of Adult HIV-Infected Individuals in Hanoi, 2007-2014
- PMID: 26939050
- PMCID: PMC4777554
- DOI: 10.1371/journal.pone.0150781
Incidence of AIDS-Defining Opportunistic Infections and Mortality during Antiretroviral Therapy in a Cohort of Adult HIV-Infected Individuals in Hanoi, 2007-2014
Abstract
Background: Although the prognosis for HIV-infected individuals has improved after antiretroviral therapy (ART) scale-up, limited data exist on the incidence of AIDS-defining opportunistic infections (ADIs) and mortality during ART in resource-limited settings.
Methods: HIV-infected adults in two large hospitals in urban Hanoi were enrolled to the prospective cohort, from October 2007 through December 2013. Those who started ART less than one year before enrollment were assigned to the survival analysis. Data on ART history and ADIs were collected retrospectively at enrollment and followed-up prospectively until April 2014.
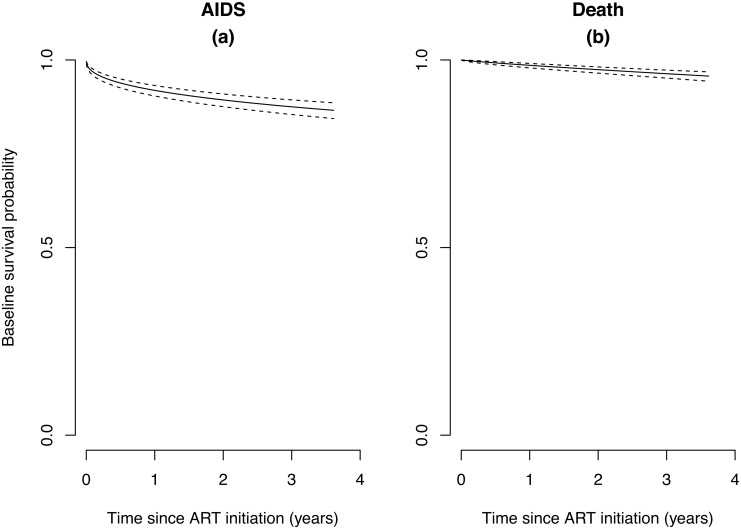
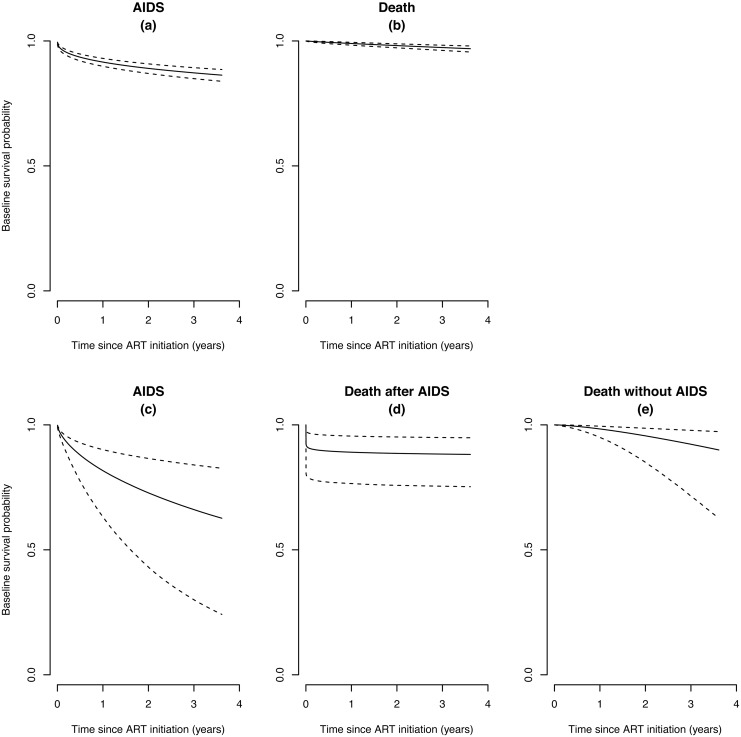
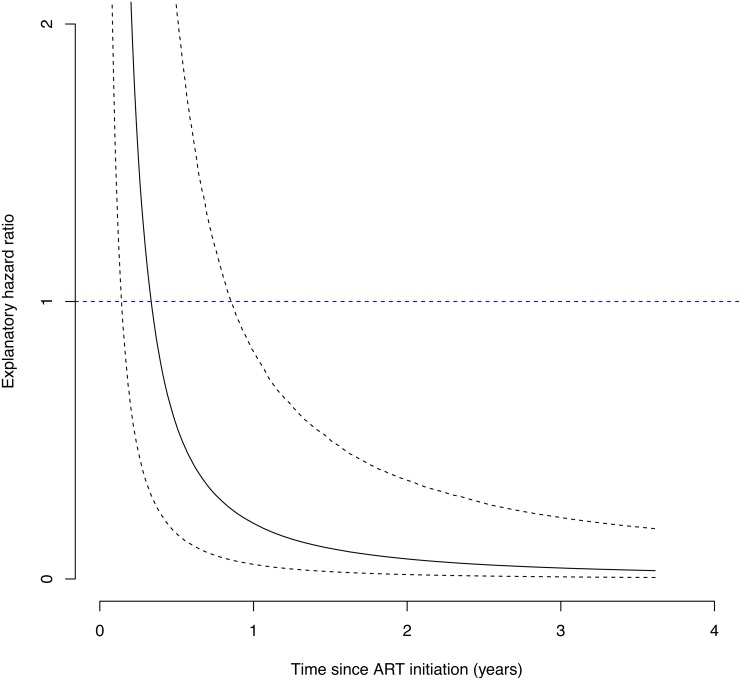
Results: Of 2,070 cohort participants, 1,197 were eligible for analysis and provided 3,446 person-years (PYs) of being on ART. Overall, 161 ADIs episodes were noted at a median of 3.20 months after ART initiation (range 0.03-75.8) with an incidence 46.7/1,000 PYs (95% confidence interval [CI] 39.8-54.5). The most common ADI was tuberculosis with an incidence of 29.9/1,000 PYs. Mortality after ART initiation was 8.68/1,000 PYs and 45% (19/45) died of AIDS-related illnesses. Age over 50 years at ART initiation was significantly associated with shorter survival after controlling for baseline CD4 count, but neither having injection drug use (IDU) history nor previous ADIs were associated with poor survival. Semi-competing risks analysis in 951 patients without ADIs history prior to ART showed those who developed ADIs after starting ART were at higher risk of death in the first six months than after six months.
Conclusion: ADIs were not rare in spite of being on effective ART. Age over 50 years, but not IDU history, was associated with shorter survival in the cohort. This study provides in-depth data on the prognosis of patients on ART in Vietnam during the first decade of ART scale-up.
Conflict of interest statement
Figures
References
-
- Braitstein P, Brinkhof MW, Dabis F, Schechter M, Boulle A, Miotti P, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367(9513):817–824. Epub 2006/03/15. 10.1016/s0140-6736(06)68337-2 - DOI - PubMed
-
- Marazzi MC, Liotta G, Germano P, Guidotti G, Altan AD, Ceffa S, et al. Excessive early mortality in the first year of treatment in HIV type 1-infected patients initiating antiretroviral therapy in resource-limited settings. AIDS Res Hum Retroviruses. 2008;24(4):555–560. 10.1089/aid.2007.0217 - DOI - PubMed
-
- Boulle A, Schomaker M, May MT, Hogg RS, Shepherd BE, Monge S, et al. Mortality in patients with HIV-1 infection starting antiretroviral therapy in South Africa, Europe, or North America: a collaborative analysis of prospective studies. PLoS Med. 2014;11(9):e1001718 10.1371/journal.pmed.1001718 - DOI - PMC - PubMed
-
- May MT, Sterne JA, Costagliola D, Sabin CA, Phillips AN, Justice AC, et al. HIV treatment response and prognosis in Europe and North America in the first decade of highly active antiretroviral therapy: a collaborative analysis. Lancet. 2006;368(9534):451–458. 10.1016/s0140-6736(06)69152-6 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
