

Vena Caval Filter Utilization and Outcomes in Pulmonary Embolism: Medicare Hospitalizations From 1999 to 2010
- PMID: 26940921
- PMCID: PMC5322943
- DOI: 10.1016/j.jacc.2015.12.028
Vena Caval Filter Utilization and Outcomes in Pulmonary Embolism: Medicare Hospitalizations From 1999 to 2010
Abstract
Background: Inferior vena caval filters (IVCFs) may prevent recurrent pulmonary embolism (PE). Despite uncertainty about their net benefit, patterns of use and outcomes of these devices in contemporary practice are unknown.
Objectives: The authors determined the trends in utilization rates and outcomes of IVCF placement in patients with PE and explored regional variations in use in the United States.
Methods: In a national cohort study of all Medicare fee-for-service beneficiaries ≥65 years of age with principal discharge diagnoses of PE between 1999 and 2010, rates of IVCF placement per 100,000 beneficiary-years and per 1,000 patients with PE were determined. The 30-day and 1-year mortality rates after IVCF placement were also investigated.
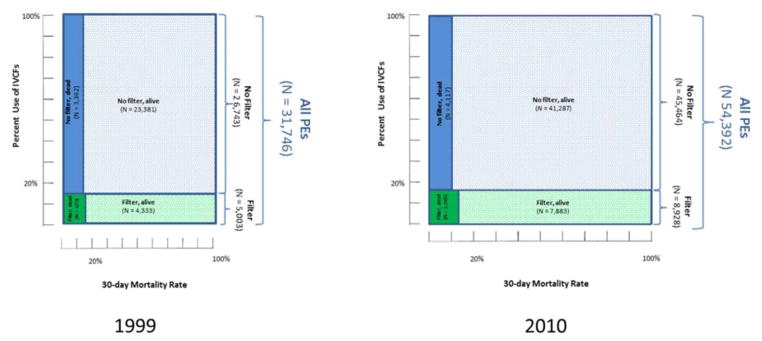
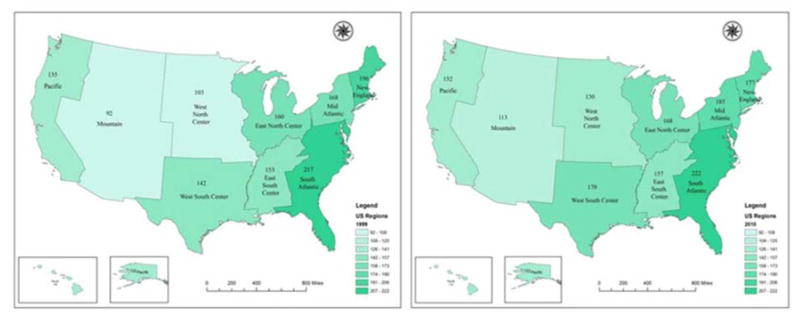
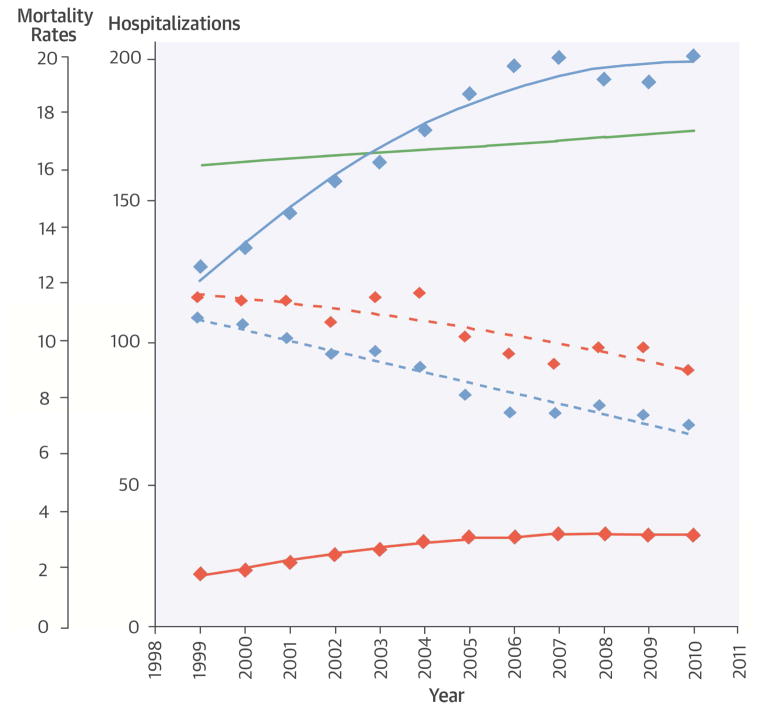
Results: Among 556,658 patients hospitalized with PE, 94,427 underwent IVCF placement. Between 1999 and 2010, the number of PE hospitalizations with IVCF placement increased from 5,003 to 8,928, representing an increase in the rate per 100,000 beneficiary-years from 19.0 to 32.5 (p < 0.001 for both). As the total number of PE hospitalizations increased (from 31,746 in 1999 to 54,392 in 2010), the rate of IVCF placement per 1,000 PE hospitalizations did not change significantly (from 157.6 to 164.1, p = 0.11). Results were consistent across demographic subgroups, although IVCF use was higher in blacks and patients ≥85 years of age. IVCF utilization varied widely across regions, with the highest rate in the South Atlantic region and the lowest rate in the Mountain region.
Conclusions: In a period of increasing PE hospitalizations among Medicare fee-for-service beneficiaries, IVCF placement increased as utilization rates in patients with PE remained greater than 15%. Mortality associated with PE hospitalizations is declining, regardless of IVCF use.
Keywords: deep vein thrombosis; mortality; trends.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Is There a Subgroup of PE Patients Who Benefit From Inferior Vena Cava Filters?J Am Coll Cardiol. 2016 Mar 8;67(9):1036-1037. doi: 10.1016/j.jacc.2015.12.029. J Am Coll Cardiol. 2016. PMID: 26940922 No abstract available.
References
-
- Decousus H, Leizorovicz A, Parent F, et al. A clinical trial of vena caval filters in the prevention of pulmonary embolism in patients with proximal deep-vein thrombosis. Prevention du Risque d’Embolie Pulmonaire par Interruption Cave Study Group. N Engl J Med. 1998;338:409–15. - PubMed
-
- Group PS. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d’Embolie Pulmonaire par Interruption Cave) randomized study. Circulation. 2005;112:416–22. - PubMed
-
- Mismetti P, Laporte S, Pellerin O, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone on risk of recurrent pulmonary embolism: a randomized clinical trial. JAMA. 2015;313:1627–35. - PubMed
-
- Barginear MF, Gralla RJ, Bradley TP, et al. Investigating the benefit of adding a vena cava filter to anticoagulation with fondaparinux sodium in patients with cancer and venous thromboembolism in a prospective randomized clinical trial. Support Care Cancer. 2012;20:2865–72. - PubMed
-
- Jaff MR, McMurtry MS, Archer SL, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123:1788–830. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
