

Leukocytes Link Local and Systemic Inflammation in Ischemic Cardiovascular Disease: An Expanded "Cardiovascular Continuum"
- PMID: 26940931
- PMCID: PMC4779182
- DOI: 10.1016/j.jacc.2015.12.048
Leukocytes Link Local and Systemic Inflammation in Ischemic Cardiovascular Disease: An Expanded "Cardiovascular Continuum"
Abstract
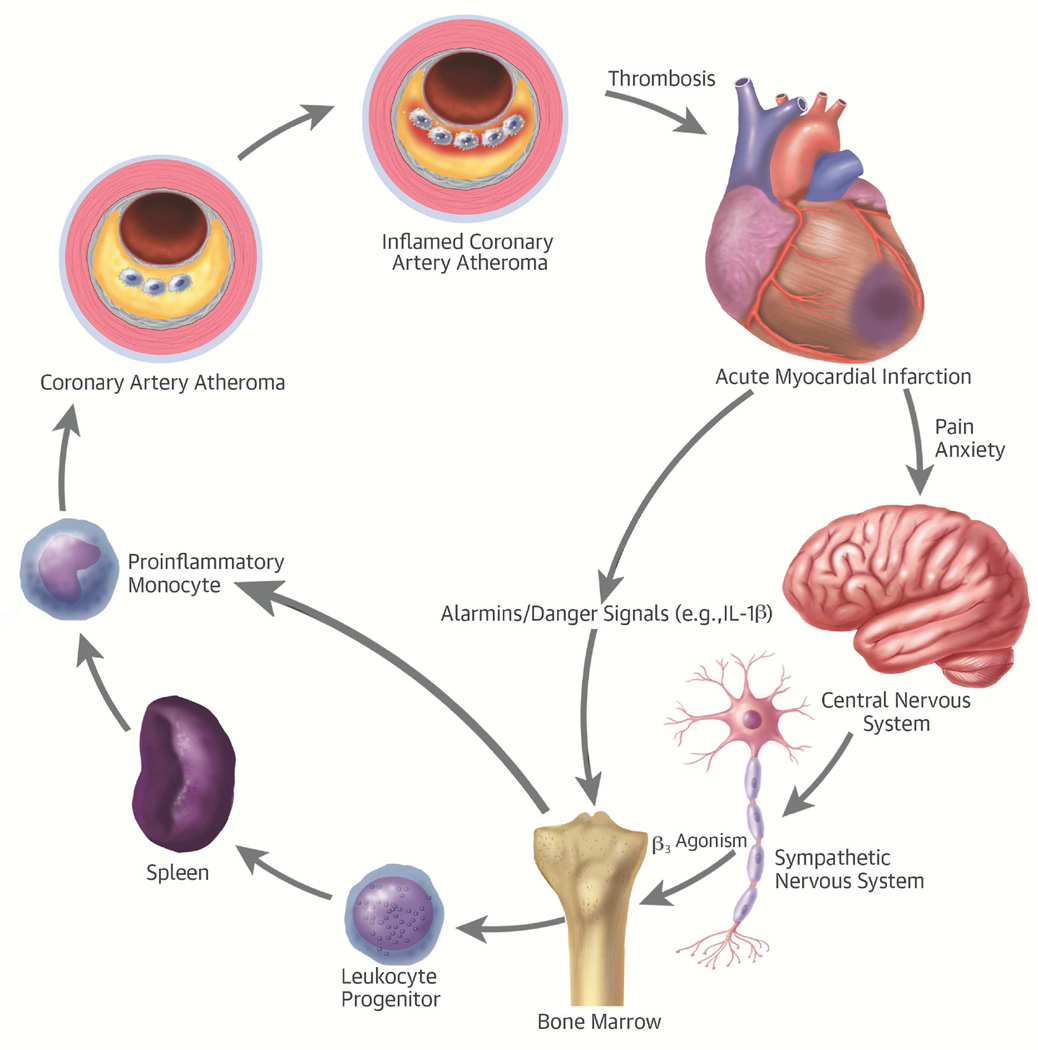
Physicians have traditionally viewed ischemic heart disease in a cardiocentric manner: plaques grow in arteries until they block blood flow, causing acute coronary and other ischemic syndromes. Recent research provides new insight into the integrative biology of inflammation as it contributes to ischemic cardiovascular disease. These results have revealed hitherto unsuspected inflammatory signaling networks at work in these disorders that link the brain, autonomic nervous system, bone marrow, and spleen to the atherosclerotic plaque and to the infarcting myocardium. A burgeoning clinical published data indicates that such inflammatory networks-far from a mere laboratory curiosity-operate in our patients and can influence aspects of ischemic cardiovascular disease that determine decisively clinical outcomes. These new findings enlarge the circle of the traditional "cardiovascular continuum" beyond the heart and vessels to include the nervous system, the spleen, and the bone marrow.
Keywords: acute coronary syndromes; myocardial infarction; white blood cells.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Networks Between the Sympathetic Nervous System and Immune System in Atherosclerosis.J Am Coll Cardiol. 2016 Jul 26;68(4):431-2. doi: 10.1016/j.jacc.2016.04.049. J Am Coll Cardiol. 2016. PMID: 27443444 No abstract available.
-
Reply: The Networks Between the Sympathetic Nervous System and Immune System in Atherosclerosis.J Am Coll Cardiol. 2016 Jul 26;68(4):432. doi: 10.1016/j.jacc.2016.05.017. J Am Coll Cardiol. 2016. PMID: 27443446 No abstract available.
References
-
- Virchow R. Cellular Pathology. London, UK: John Churchill; 1858.
-
- Virchow R. Cellular pathology. As based upon physiological and pathological histology. Lecture XVI--Atheromatous affection of arteries. 1858. Nutr Rev. 1989;47:23–25. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
