

A multi-centre open-label randomised non-inferiority trial comparing watchful waiting to antibiotic treatment for acute otitis media without perforation in low-risk urban Aboriginal and Torres Strait Islander children (the WATCH trial): study protocol for a randomised controlled trial
- PMID: 26941013
- PMCID: PMC4778283
- DOI: 10.1186/s13063-016-1247-y
A multi-centre open-label randomised non-inferiority trial comparing watchful waiting to antibiotic treatment for acute otitis media without perforation in low-risk urban Aboriginal and Torres Strait Islander children (the WATCH trial): study protocol for a randomised controlled trial
Abstract
Background: Treatment guidelines recommend watchful waiting for children older than 2 years with acute otitis media (AOM) without perforation, unless they are at high risk of complications. The high prevalence of chronic suppurative otitis media (CSOM) in remote Aboriginal and Torres Strait Islander communities leads these children to be classified as high risk. Urban Aboriginal and Torres Strait Islander children are at lower risk of complications, but evidence to support the subsequent recommendation for watchful waiting in this population is lacking.
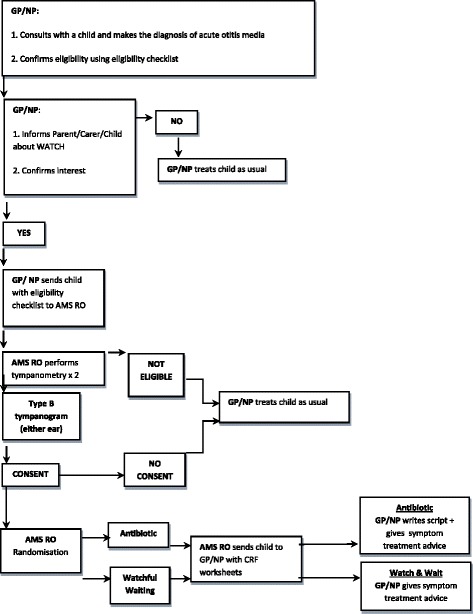
Methods/design: This non-inferiority multi-centre randomised controlled trial will determine whether watchful waiting is non-inferior to immediate antibiotics for urban Aboriginal and Torres Strait Islander children with AOM without perforation. Children aged 2 - 16 years with AOM who are considered at low risk for complications will be recruited from six participating urban primary health care services across Australia. We will obtain informed consent from each participant or their guardian. The primary outcome is clinical resolution on day 7 (no pain, no fever of at least 38 °C, no bulging eardrum and no complications of AOM such as perforation or mastoiditis) as assessed by general practitioners or nurse practitioners. Participants and outcome assessors will not be blinded to treatment. With a sample size of 198 children in each arm, we have 80 % power to detect a non-inferiority margin of up to 10 % at a significance level of 5 %, assuming clinical improvement of at least 80 % in both groups. Allowing for a 20 % dropout rate, we aim to recruit 495 children. We will analyse both by intention-to-treat and per protocol. We will assess the cost- effectiveness of watchful waiting compared to immediate antibiotic prescription. We will also report on the implementation of the trial from the perspectives of parents/carers, health professionals and researchers.
Discussion: The trial will provide evidence for the safety and effectiveness of watchful waiting for the management of AOM in Aboriginal and Torres Strait Islander children living in urban settings who are considered to be at low risk of complications.
Trial registration: The trial is registered with Australia New Zealand Clinical Trials Registry ( ACTRN12613001068752 ). Date of registration: 24 September 2013.
References
-
- Charles J, Pan Y, Britt H. Trends in childhood illness and treatment in Australian general practice, 1971−2001. Med J Aust. 2004;180(5):216–9. - PubMed
-
- Darwin Otitis Guidelines Group & Office for Aboriginal and Torres Strait Islander Health Otitis Media Technical Advisory Group . Recommendations for clinical care guidelines on the management of otitis media in Aboriginal & Torres Strait Islander populations. Canberra: Commonwealth of Australia; 2010.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
