

T-Cell Immunity to Influenza in Older Adults: A Pathophysiological Framework for Development of More Effective Vaccines
- PMID: 26941738
- PMCID: PMC4766518
- DOI: 10.3389/fimmu.2016.00041
T-Cell Immunity to Influenza in Older Adults: A Pathophysiological Framework for Development of More Effective Vaccines
Abstract
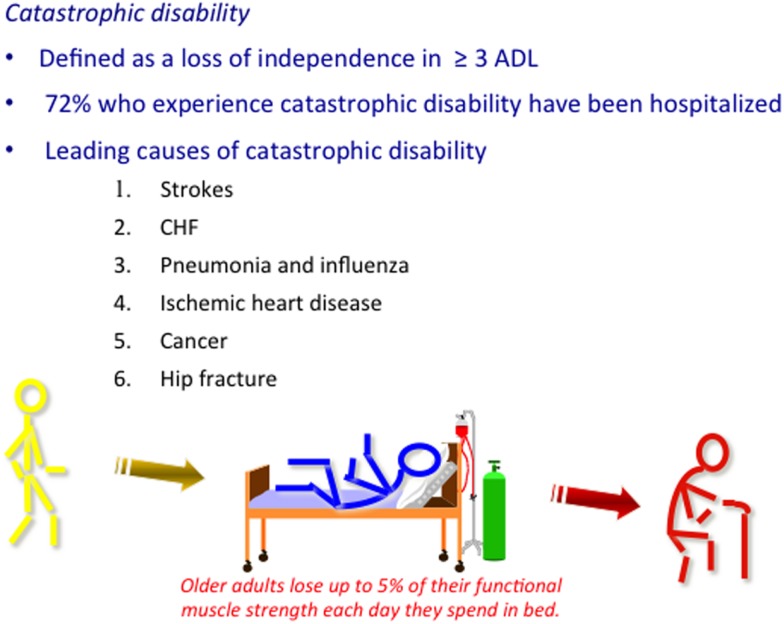
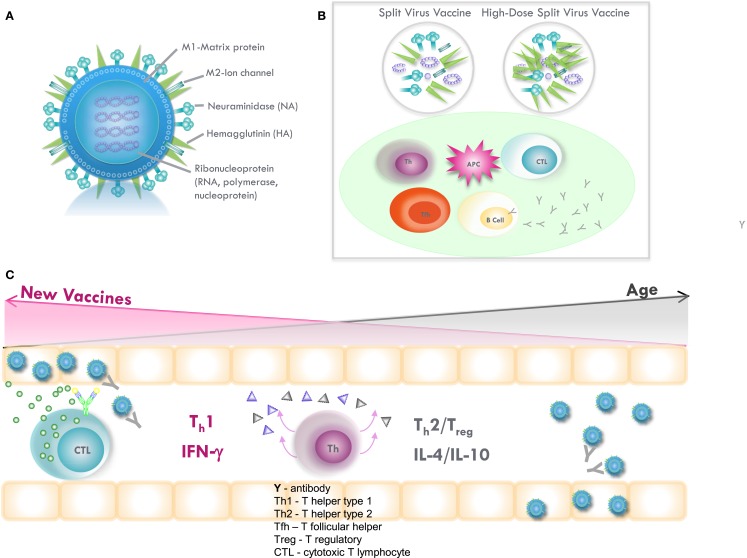
One of the most profound public health consequences of immune senescence is reflected in an increased susceptibility to influenza and other acute respiratory illnesses, as well as a loss of influenza vaccine effectiveness in older people. Common medical conditions and mental and psychosocial health issues as well as degree of frailty and functional dependence accelerate changes associated with immune senescence. All contribute to the increased risk for complications of influenza infection, including pneumonias, heart diseases, and strokes that lead to hospitalization, disability, and death in the over 65 population. Changes in mucosal barrier mechanisms and both innate and adaptive immune functions converge in the reduced response to influenza infection, and lead to a loss of antibody-mediated protection against influenza with age. The interactions of immune senescence and reduced adaptive immune responses, persistent cytomegalovirus infection, inflammaging (chronic elevation of inflammatory cytokines), and dysregulated cytokine production, pose major challenges to the development of vaccines designed to improve T-cell-mediated immunity. In older adults, the goal of vaccination is more realistically targeted to providing clinical protection against disease rather than to inducing sterilizing immunity to infection. Standard assays of antibody titers correlate with protection against influenza illness but do not detect important changes in cellular immune mechanisms that correlate with vaccine-mediated protection against influenza in older people. This article will discuss: (i) the burden of influenza in older adults and how this relates to changes in T-cell function, (ii) age-related changes in different T-cell subsets and immunologic targets for improved influenza vaccine efficacy in older, and (iii) the development of correlates of clinical protection against influenza disease to expedite the process of new vaccine development for the 65 and older population. Ultimately, these efforts will address the public health need for improved protection against influenza in older adults and "vaccine preventable disability."
Keywords: antibody; cell-mediated immunity; immunosenescence; influenza; vaccination.
Figures
Similar articles
-
Influenza vaccine responses in older adults.Ageing Res Rev. 2011 Jul;10(3):379-88. doi: 10.1016/j.arr.2010.10.008. Epub 2010 Nov 3. Ageing Res Rev. 2011. PMID: 21055484 Free PMC article. Review.
-
Influenza Vaccination: Accelerating the Process for New Vaccine Development in Older Adults.Interdiscip Top Gerontol Geriatr. 2020;43:98-112. doi: 10.1159/000504478. Epub 2020 Apr 9. Interdiscip Top Gerontol Geriatr. 2020. PMID: 32305974 Review.
-
Immunologic correlates of protection and potential role for adjuvants to improve influenza vaccines in older adults.Expert Rev Vaccines. 2013 Jul;12(7):759-66. doi: 10.1586/14760584.2013.811193. Expert Rev Vaccines. 2013. PMID: 23885821 Review.
-
Impact of Aging and Cytomegalovirus on Immunological Response to Influenza Vaccination and Infection.Front Immunol. 2017 Jul 17;8:784. doi: 10.3389/fimmu.2017.00784. eCollection 2017. Front Immunol. 2017. PMID: 28769922 Free PMC article. Review.
-
Cell-Mediated Immune Response to Influenza Using Ex Vivo Stimulation and Assays of Cytokine and Granzyme B Responses.Methods Mol Biol. 2015;1343:121-41. doi: 10.1007/978-1-4939-2963-4_11. Methods Mol Biol. 2015. PMID: 26420714
Cited by
-
New Insights into the Generation of CD4 Memory May Shape Future Vaccine Strategies for Influenza.Front Immunol. 2016 Apr 11;7:136. doi: 10.3389/fimmu.2016.00136. eCollection 2016. Front Immunol. 2016. PMID: 27148257 Free PMC article. Review.
-
Modulation of Primary Immune Response by Different Vaccine Adjuvants.Front Immunol. 2016 Oct 17;7:427. doi: 10.3389/fimmu.2016.00427. eCollection 2016. Front Immunol. 2016. PMID: 27781036 Free PMC article.
-
Cellular Immune Response after Vaccination in Patients with Cancer-Review on Past and Present Experiences.Vaccines (Basel). 2022 Jan 25;10(2):182. doi: 10.3390/vaccines10020182. Vaccines (Basel). 2022. PMID: 35214642 Free PMC article. Review.
-
Network Topology of Biological Aging and Geroscience-Guided Approaches to COVID-19.Front Aging. 2021 Jul;2:695218. doi: 10.3389/fragi.2021.695218. Epub 2021 Jul 23. Front Aging. 2021. PMID: 35128530 Free PMC article.
-
Human T cell immunosenescence and inflammation in aging.J Leukoc Biol. 2017 Oct;102(4):977-988. doi: 10.1189/jlb.3RI0716-335R. Epub 2017 Jul 21. J Leukoc Biol. 2017. PMID: 28733462 Free PMC article. Review.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources