

Surgical technology and pharmacology of hyperthermic perioperative chemotherapy
- PMID: 26941982
- PMCID: PMC4754302
- DOI: 10.3978/j.issn.2078-6891.2015.105
Surgical technology and pharmacology of hyperthermic perioperative chemotherapy
Abstract
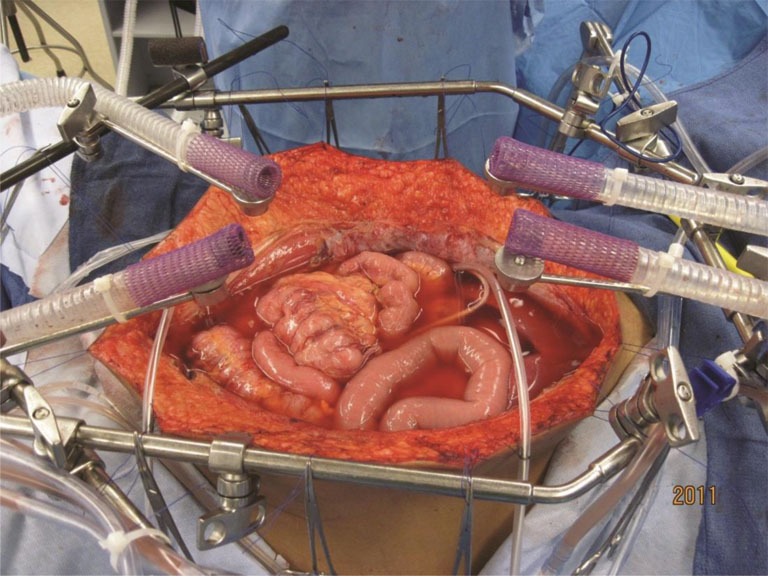
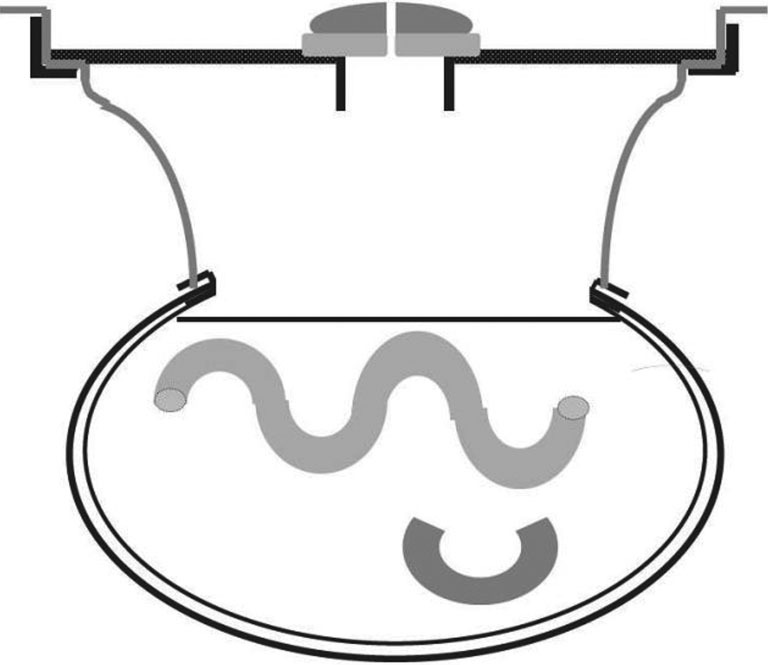
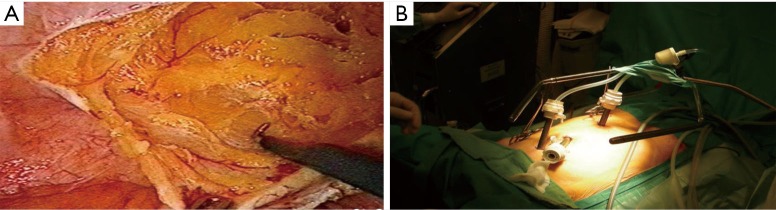
Although cytoreductive surgery (CRS) and hyperthermic perioperative chemotherapy (HIPEC) have not been shown to be effective by themselves, as a combined treatment they are now standard of care for peritoneal metastases from appendiceal cancer and from colorectal cancer as well as peritoneal mesothelioma. The timing of the HIPEC in relation to the CRS is crucial in that the HIPEC is to destroy minimal residual disease that remains following the CRS and prevent microscopic tumor emboli within the abdomen and pelvis from implanting within the resection site, within fibrinous clot, or within blood clot. Proper selection of chemotherapy agents is crucial to the long-term benefit of CRS and HIPEC. One must consider the response expected with the cancer chemotherapy agent, its area under the curve (AUC) ratio indicating the amount of dose intensity within the peritoneal space, and the drug retention within the peritoneal space for a prolonged exposure. Hyperthermia will augment the cytotoxicity of the cancer chemotherapy agents and improve drug penetration. Irrigation techniques should not be overlooked as an important means of reducing the cancer cell burden within the abdomen and pelvis. Multiple technologies for HIPEC exist and these have advantages and disadvantages. The techniques vary from a totally open technique with a vapor barrier over the open abdominal space to a totally closed technique whereby the HIPEC is administered at the completion of the surgical procedure. The open techniques depend on a table-mounted retractor for suspension of the skin edges allowing a reservoir to occur within the abdomen and pelvis. There are nearly a dozen commercially available hyperthermia pumps, all of which seem to perform adequately for HIPEC although there is a variable degree of convenience and documentation of the HIPEC procedure. As the management of peritoneal metastases has progressed over three decades, early cases are now seen in which a laparoscopic CRS and HIPEC may be appropriate. Also, prophylactic use of laparoscopic HIPEC with perforated appendiceal malignancies and T4 colon cancers may be appropriate.
Keywords: Peritoneal metastases; carcinomatosis; hyperthermic perioperative chemotherapy (HIPEC); irrigation; laparoscopic cytoreductive surgery; laparoscopy; peritoneal mesothelioma.
Conflict of interest statement
Figures

References
-
- Sugarbaker PH. Pseudomyxoma peritonei and peritoneal metastases from appendiceal malignancy. In: Sugarbaker PH, editor. Cytoreductive Surgery & Perioperative Chemotherapy for Peritoneal Surface Malignancy. Textbook and Video Atlas. Woodbury: Cine-Med Publishing, 2012:57-78.
-
- Glehen O, Gilly FN, Boutitie F, et al. Toward curative treatment of peritoneal carcinomatosis from nonovarian origin by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy: a multi-institutional study of 1,290 patients. Cancer 2010;116:5608-18. - PubMed
-
- Bakrin N, Bereder JM, Decullier E, et al. Peritoneal carcinomatosis treated with cytoreductive surgery and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) for advanced ovarian carcinoma: a French multicentre retrospective cohort study of 566 patients. Eur J Surg Oncol 2013;39:1435-43. - PubMed
-
- Spiliotis J, Halkia E, Lianos E, et al. Cytoreductive surgery and HIPEC in recurrent epithelial ovarian cancer: a prospective randomized phase III study. Ann Surg Oncol 2015;22:1570-5. - PubMed
-
- Glehen O, Mithieux F, Osinsky D, et al. Surgery combined with peritonectomy procedures and intraperitoneal chemohyperthermia in abdominal cancers with peritoneal carcinomatosis: a phase II study. J Clin Oncol 2003;21:799-806. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials