

Timeline of History of Hypertension Treatment
- PMID: 26942184
- PMCID: PMC4763852
- DOI: 10.3389/fcvm.2016.00003
Timeline of History of Hypertension Treatment
Abstract
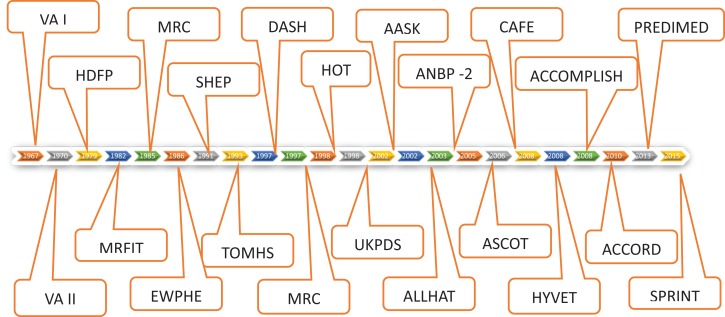
It is surprising that only about 50 years ago hypertension was considered an essential malady and not a treatable condition. Introduction of thiazide diuretics in late 50s made some headway in successful treatment of hypertension and ambitious multicenter VA co-operative study (phase 1 and 2) started in 1964 for diastolic hypertension ranging between 90 and 129 mmHg and completed by 1971 established for the first time that treating diastolic hypertension reduced CV events such as stroke and heart failure and improved mortality. In the following decade, these results were confirmed for the wider US and non-US population, including women and goal-oriented BP treatment to diastolic 90 became the standard therapy recommendation. But isolated systolic hypertension (accounting for two-thirds of the 70 million hypertensive population in USA alone) was not considered treatable until 1991 when SHEP study (systolic hypertension in elderly program) was completed and showed tremendous benefits of treating systolic BP over 160 mmHg using only a simple regimen using small dose chlorthalidone with addition of atenolol if needed. In the next two decades, ALLHAT and other studies examined the comparability of outcomes with use of different classes and combinations of antihypertensive drugs. Although diastolic BP goal was established as 90 in the late 70s and later confirmed by HOT study, the goal BP for systolic hypertension was not settled until very recently with completion of SPRINT study. ACCORD study showed no significant difference in outcome with sys 140 vs. 120 in diabetics. But recently completed SPRINT study with somewhat similar protocol as in ACCORD but in non-diabetic showed almost one-quarter reduction in all-cause mortality and one-third reduction of CV events with systolic BP goal 120.
Keywords: history; hypertension; multicenter trial; randomized controlled trials; treatment outcome.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources