

Stereotactic body radiotherapy for metastatic spinal sarcoma: a detailed patterns-of-failure study
- PMID: 26943256
- PMCID: PMC5551386
- DOI: 10.3171/2015.11.SPINE151059
Stereotactic body radiotherapy for metastatic spinal sarcoma: a detailed patterns-of-failure study
Abstract
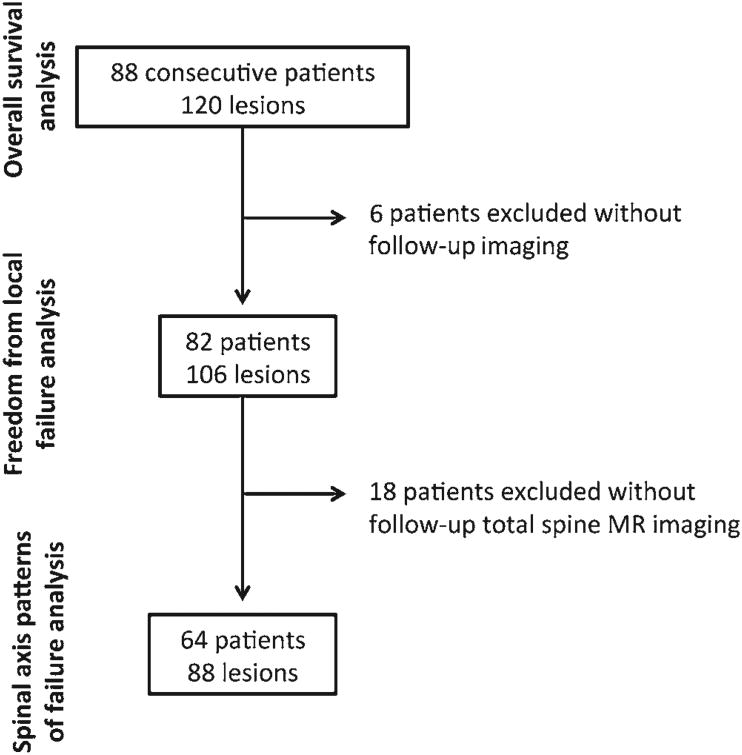
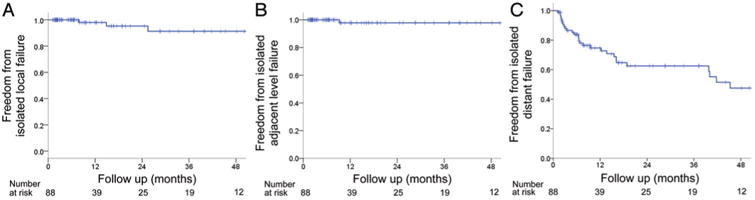
OBJECTIVE The aim of this study was to report the first detailed analysis of patterns of failure within the spinal axis of patients treated with stereotactic body radiotherapy (SBRT) for sarcoma spine metastases. METHODS Between 2005 and 2012, 88 consecutive patients with metastatic sarcoma were treated with SBRT for 120 spinal lesions. Seventy-one percent of patients were enrolled on prospective institutional protocols. For patients who underwent routine posttreatment total-spine MRI (64 patients, 88 lesions), each site of progression within the entire spinal axis was mapped in relation to the treated lesion. Actuarial rates of local-, adjacent-, and distant-segment failure-free survival (FFS) were calculated using the Kaplan-Meier method. RESULTS The median follow-up for the cohort was 14.4 months, with 81.7% of patients followed up until death. The 12-month actuarial rate of local FFS was 85.9%; however, 83.3% of local failures occurred in conjunction with distant-segment failures. The 12-month actuarial rates of isolated local-, adjacent-, and distant-segment FFS were 98.0%, 97.8%, and 74.7%, respectively. Of patients with any spinal progression (n = 55), only 25.5% (n = 14) had progression at a single vertebral level, with 60.0% (n = 33) having progression at ≥ 3 sites within the spine simultaneously. Linear regression analysis revealed a relationship of decreasing risk of failure with increasing distance from the treated index lesion (R(2) = 0.87), and 54.1% of failures occurred ≥ 5 vertebral levels away. Treatment of the index lesion with a lower biological effective dose (OR 3.2, 95% CI 1.1-9.2) and presence of local failure (OR 18.0, 95% CI 2.1-152.9) independently predicted for distant spine failure. CONCLUSIONS Isolated local- and adjacent-segment failures are exceptionally rare for patients with metastatic sarcoma to the spine treated with SBRT, thereby affirming the treatment of the involved level only. The majority of progression within the spinal axis occurs ≥ 5 vertebral levels away. Thus, total-spine imaging is necessary for surveillance posttreatment.
Keywords: AFFS = adjacent-segment failure-free survival; DFFS = distant-segment failure-free survival; FA = flip angle; LFFS = local failure-free survival; OS = overall survival; SBRT; SBRT = stereotactic body radiotherapy; oncology; patterns of failure; sarcoma; spine metastasis; stereotactic body radiotherapy.
Figures


References
-
- Amdur RJ, Bennett J, Olivier K, Wallace A, Morris CG, Liu C, et al. A prospective, phase II study demonstrating the potential value and limitation of radiosurgery for spine metastases. Am J Clin Oncol. 2009;32:515–520. - PubMed
-
- Bilsky M, Smith M. Surgical approach to epidural spinal cord compression. Hematol Oncol Clin North Am. 2006;20:1307–1317. - PubMed
-
- Bilsky MH, Gerszten P, Laufer I, Yamada Y. Radiation for primary spine tumors. Neurosurg Clin N Am. 2008;19:119–123. - PubMed
-
- Boriani S, Saravanja D, Yamada Y, Varga PP, Biagini R, Fisher CG. Challenges of local recurrence and cure in low grade malignant tumors of the spine. Spine (Phila Pa 1976) 2009;34(22 Suppl):S48–S57. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
