

Analysis of Lung Microbiota in Bronchoalveolar Lavage, Protected Brush and Sputum Samples from Subjects with Mild-To-Moderate Cystic Fibrosis Lung Disease
- PMID: 26943329
- PMCID: PMC4778801
- DOI: 10.1371/journal.pone.0149998
Analysis of Lung Microbiota in Bronchoalveolar Lavage, Protected Brush and Sputum Samples from Subjects with Mild-To-Moderate Cystic Fibrosis Lung Disease
Abstract
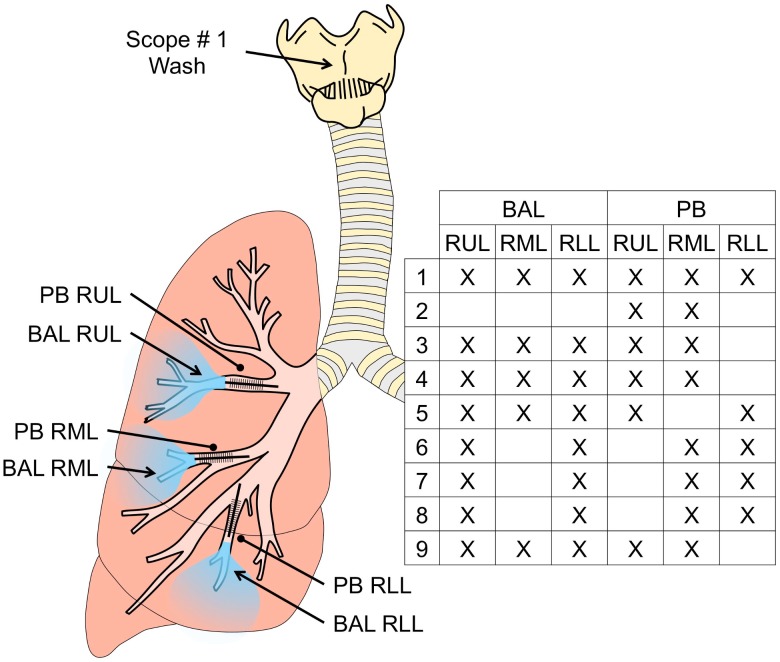
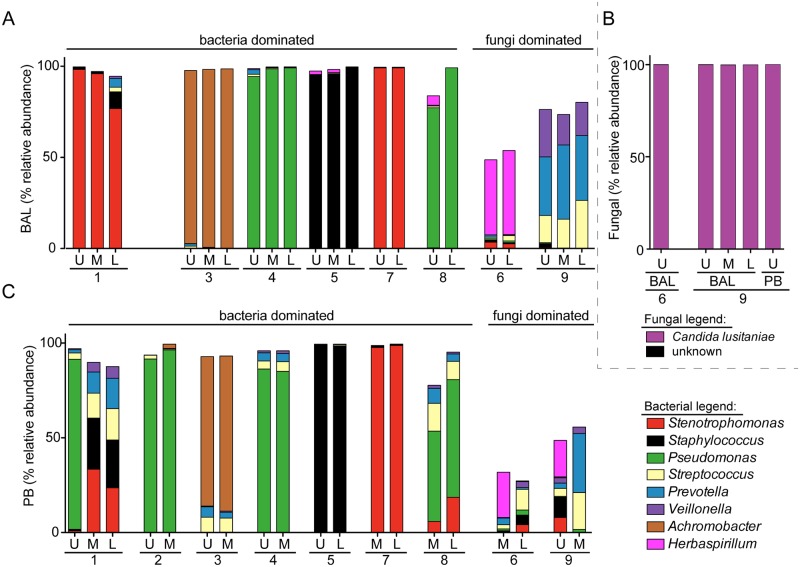
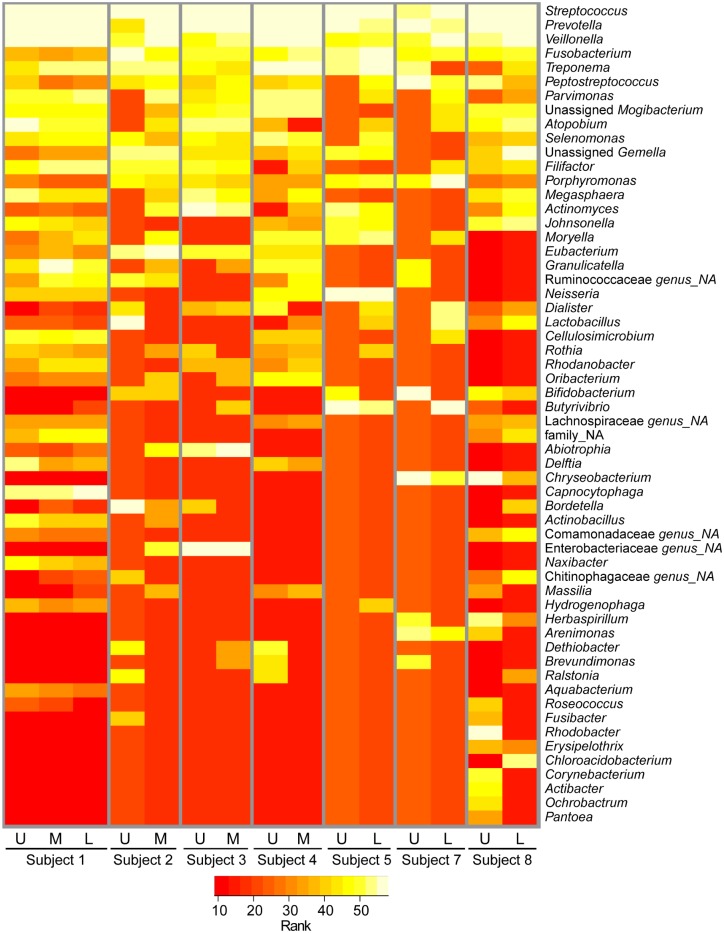
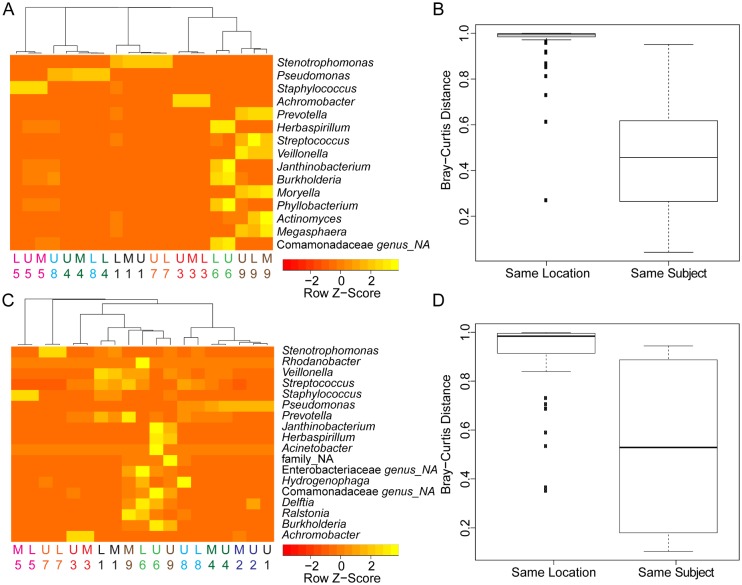
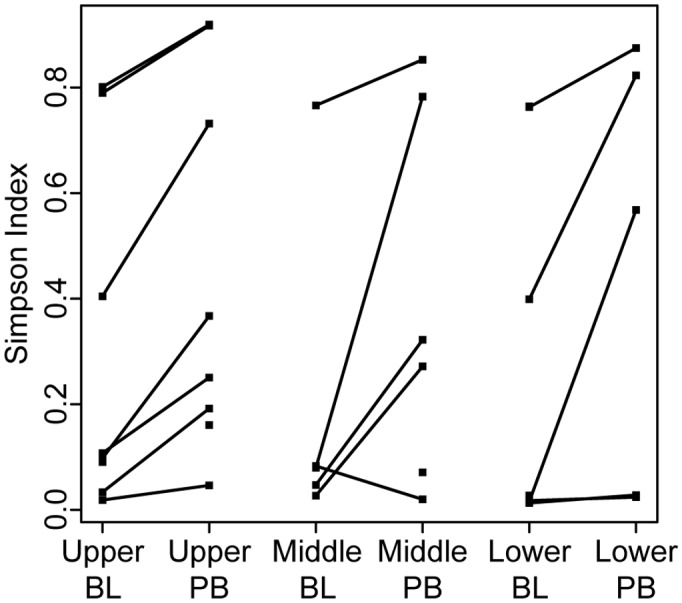
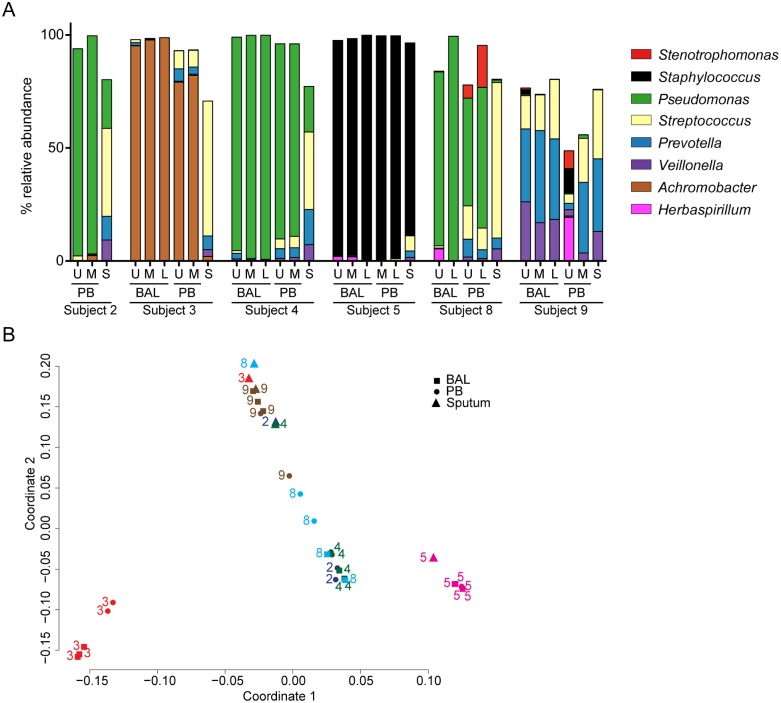
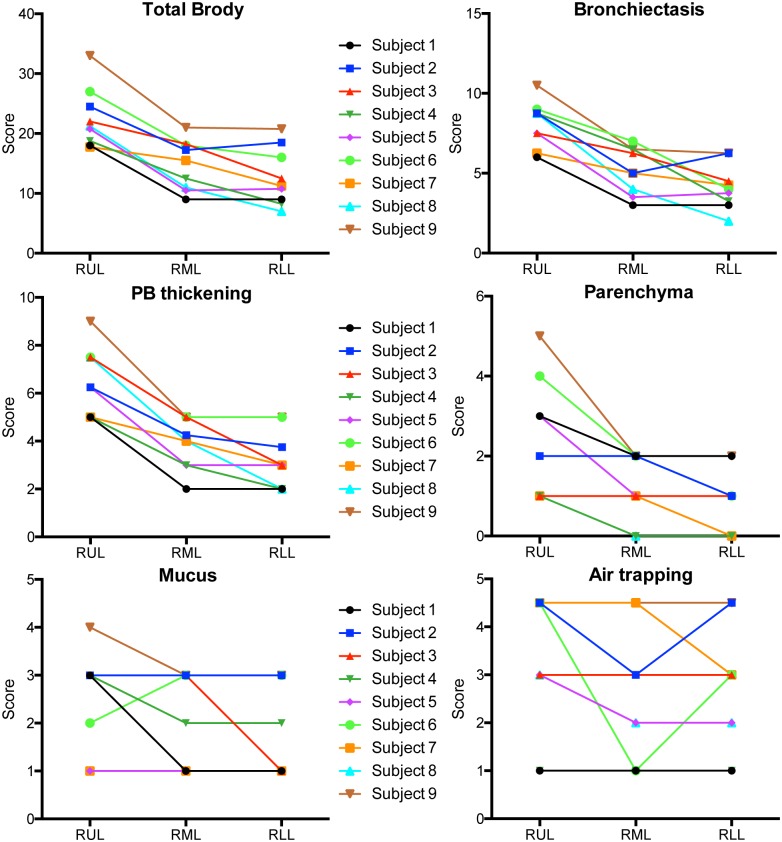
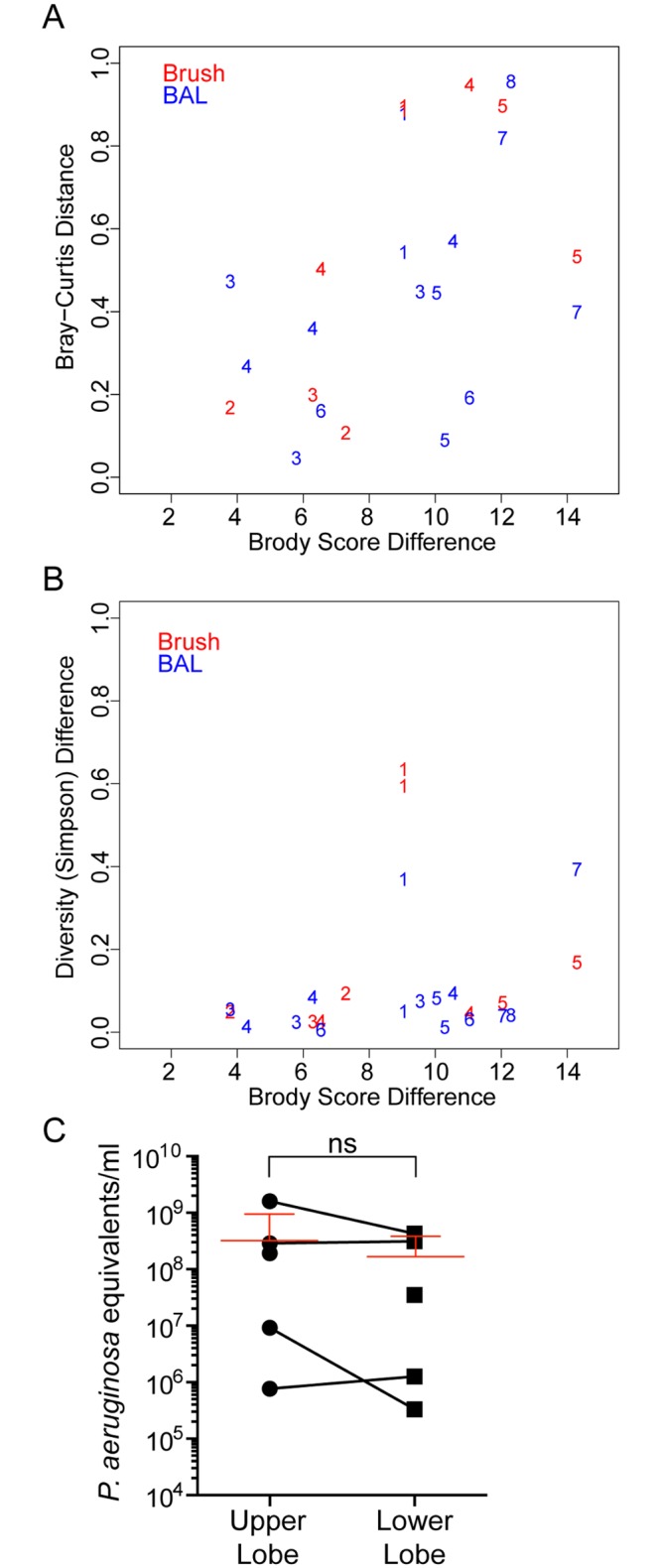
Individuals with cystic fibrosis (CF) often acquire chronic lung infections that lead to irreversible damage. We sought to examine regional variation in the microbial communities in the lungs of individuals with mild-to-moderate CF lung disease, to examine the relationship between the local microbiota and local damage, and to determine the relationships between microbiota in samples taken directly from the lung and the microbiota in spontaneously expectorated sputum. In this initial study, nine stable, adult CF patients with an FEV1>50% underwent regional sampling of different lobes of the right lung by bronchoalveolar lavage (BAL) and protected brush (PB) sampling of mucus plugs. Sputum samples were obtained from six of the nine subjects immediately prior to the procedure. Microbial community analysis was performed on DNA extracted from these samples and the extent of damage in each lobe was quantified from a recent CT scan. The extent of damage observed in regions of the right lung did not correlate with specific microbial genera, levels of community diversity or composition, or bacterial genome copies per ml of BAL fluid. In all subjects, BAL fluid from different regions of the lung contained similar microbial communities. In eight out of nine subjects, PB samples from different regions of the lung were also similar in microbial community composition, and were similar to microbial communities in BAL fluid from the same lobe. Microbial communities in PB samples were more diverse than those in BAL samples, suggesting enrichment of some taxa in mucus plugs. To our knowledge, this study is the first to examine the microbiota in different regions of the CF lung in clinically stable individuals with mild-to-moderate CF-related lung disease.
Conflict of interest statement
Figures
References
-
- Simanovsky N, Cohen-Cymberknoh M, Shoseyov D, Gileles-Hillel A, Wilschanski M, Kerem E, et al. (2013) Differences in the pattern of structural abnormalities on CT in patients with cystic fibrosis and pancreatic sufficiency or insufficiency. Chest. - PubMed
-
- Meyer KC, Sharma A (1997) Regional variability of lung inflammation in cystic fibrosis. Am J Respir Crit Care Med 156: 1536–1540. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
