

Review
doi: 10.1259/bjr.20150958.
Epub 2016 Mar 24.
Dynamic ultrasound of peroneal tendon instability
Affiliations
- PMID: 26943704
- PMCID: PMC5257307
- DOI: 10.1259/bjr.20150958
Item in Clipboard
Review
Dynamic ultrasound of peroneal tendon instability
Br J Radiol.
2016 Jul.
Abstract
Ankle snapping may be caused by peroneal tendon instability. Anterior instability occurs after traumatic superior peroneal retinaculum injury, whereas peroneal tendon intrasheath subluxation is atraumatic. Whereas subluxation is mainly dynamic, ultrasound allows for the diagnosis and classification of peroneal instability because it allows for real-time exploration. The purpose of this review is to describe the anatomic and physiologic bases for peroneal instability and to heighten the role of dynamic ultrasound in the diagnosis of snapping.
Figures

An asymptomatic 24-year-old male. Ultrasound image (a) short axis at the level of the retromalleolar fibular groove and schematic drawing (b) showing slightly concave retromalleolar groove (white arrows), superior peroneal retinaculum (arrowheads), fibrocartilage ridge (star), distal muscular fibres of the peroneus brevis (PBm), peroneus brevis tendon (PBt) and peroneus longus tendon (PLt). LM, lateral malleolus; M, malleolus.

Normal anatomy of the peroneal tendons at the level of the calcaneus. Schematic drawing (a), ultrasound image (b) short axis and surgical view using tendinoscopy (c). Peroneal tendons share a common sheath before coursing with their own sheath at the level of the peroneal tubercle (Tu). Peroneus brevis (PB) is anterior to peroneal tubercle whereas peroneous longus (PL) courses within a trochlea (Tr) anterior to the retrotrochlear eminence (E).

Oden classification. Grade I: superior peroneal retinaculum (SPR) is stripped from the malleolus. Grade II: fibrous ridge is detached from the SPR. Grade III: bony avulsion is associated with SPR injury. Grade IV: posterior SPR complete tear. PB, peroneus brevis; PL, peroneus longus.

A 32-year-old male with Grade 1 superior peroneal retinaculum (SPR) tear. Ultrasound image (a) short axis at the level of the retromalleolar fibular groove and schematic drawing (b) showing SPR (arrows) which is stripped (double headed arrows) from the lateral malleolus. Note the intact fibrocartilaginous ridge (star). LM, lateral malleolus; PB, peroneus brevis; PL, peroneus longus.

A 28-year-old female with dynamic subluxation of the peroneal tendons. Axial ultrasound images and schematic drawing in neutral position (a, b) and dorsiflexion (c, d) showing dynamic peroneus longus (PL) tendon subluxation (dotted curved white arrow) over the lateral malleolus. Superior peroneal retinaculum (white arrows) is stripped from the lateral malleolus (LM). PB, peroneus brevis.

A 34-year-old female with dynamic subluxation of the peroneal tendons and associated peroneus brevis (PB) tear. Axial dynamic ultrasound in neutral position (a) and dorsiflexion (b) showing subluxation of the peroneus longus (PL) through a longitudinal split tear of the PB and stripping of the superior peroneal retinaculum (white arrows).

Schematic drawing of different types of peroneal tendon intrasheath subluxation. (a) Normal position. (b) Type A: peroneus brevis (PB) and peroneus longus (PL) have reversed their location and the PL comes to lie deep to the PB. (c) Type B: subluxation of the PL through a longitudinal split tear of the PB.

A 32-year-old soccer player with intrasheath subluxation. Endoscopic view of distal muscle fibres (arrows) of the peroneus brevis (PB) before resection. PL, peroneus longus.
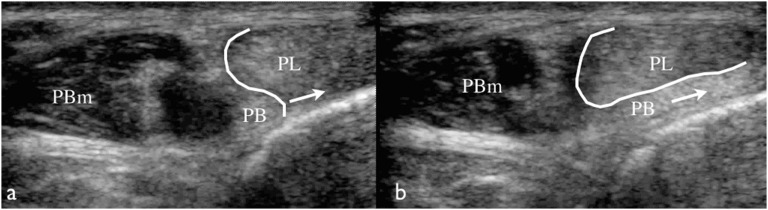
A 22-year-old-male with intrasheath subluxation. Axial dynamic ultrasound in neutral position (a) and dorsiflexion (b) showing anterior motion (arrows) of the peroneus brevis (PB) at the level of its myotendinous junction in eversion at the undersurface of the peroneus longus (PL) tendon. PBm, peroneus brevis muscle belly.
References
-
- Monteggia GB. Milan, Italy: Instituzini Chirurgiche; 1803: 336–41.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
