

Examining the effects of comorbidities on disease-modifying therapy use in multiple sclerosis
- PMID: 26944268
- PMCID: PMC4826339
- DOI: 10.1212/WNL.0000000000002543
Examining the effects of comorbidities on disease-modifying therapy use in multiple sclerosis
Abstract
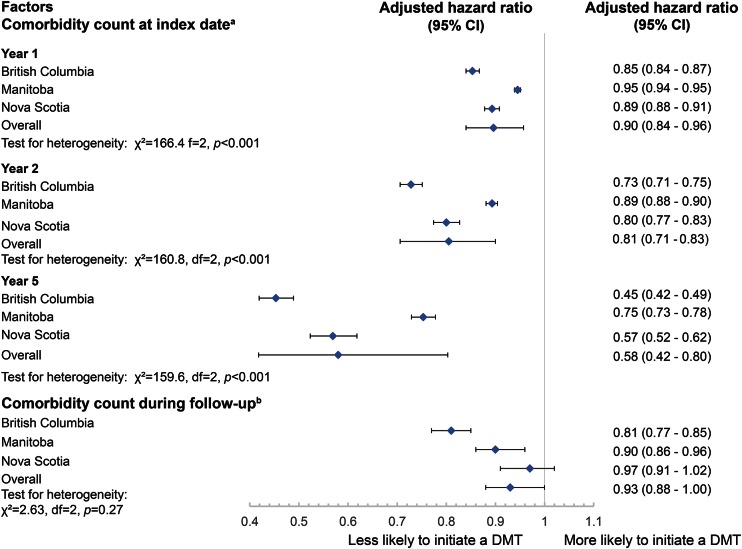
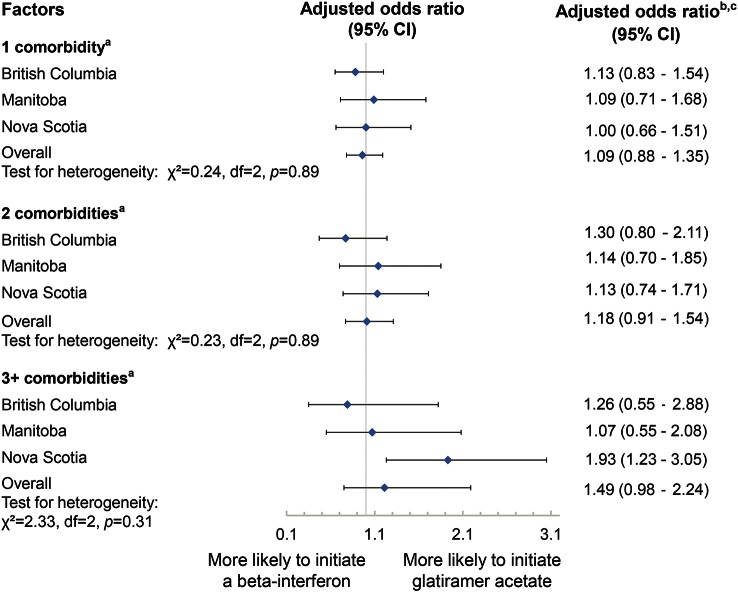
Objective: Comorbidities are common in multiple sclerosis (MS) and adversely affect health outcomes. However, the effect of comorbidity on treatment decisions in MS remains unknown. We aimed to examine the effects of comorbidity on initiation of injectable disease-modifying therapies (DMTs) and on the choice of the initial DMT in MS.
Methods: We conducted a retrospective observational analysis using population-based health administrative and linked clinical databases in 3 Canadian provinces. MS cases were defined as any individual with ≥3 diagnostic codes for MS. Cohort entry (index date) was the first recorded demyelinating disease-related claim. The outcomes included choice of initial first-line DMTs and time to initiating a DMT. Logistic and Cox regression models were used to examine the association between comorbidity status and study outcomes, adjusting for sex, age, year of index date, and socioeconomic status. Meta-analysis was used to estimate overall effects across the 3 provinces.
Results: We identified 10,698 persons with incident MS, half of whom had ≥1 comorbidities. As the total number of comorbidities increased, the likelihood of initiating a DMT decreased. Comorbid anxiety and ischemic heart disease were associated with reduced initiation of a DMT. However, patients with depression were 13% more likely to initiate a DMT compared to those without depression at the index date (adjusted hazard ratio 1.13; 95% confidence interval 1.00-1.27).
Conclusions: Comorbidities are associated with treatment decisions regarding DMTs in MS. A better understanding of the effects of comorbidity on effectiveness and safety of DMTs is needed.
© 2016 American Academy of Neurology.
Figures

References
-
- Rochon PA, Katz JN, Morrow LA, et al. Comorbid illness is associated with survival and length of hospital stay in patients with chronic disability: a prospective comparison of three comorbidity indices. Med Care 1996;34:1093–1101. - PubMed
-
- Tettey P, Simpson S, Jr, Taylor B, et al. An adverse lipid profile is associated with disability and progression in disability, in people with MS. Mult Scler 2014;20:1737–1744. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials