

Neurologic involvement in patients with atypical Chediak-Higashi disease
- PMID: 26944273
- PMCID: PMC4826336
- DOI: 10.1212/WNL.0000000000002551
Neurologic involvement in patients with atypical Chediak-Higashi disease
Erratum in
-
Neurologic involvement in patients with atypical Chediak-Higashi disease.Neurology. 2017 Feb 14;88(7):720. doi: 10.1212/WNL.0000000000003650. Neurology. 2017. PMID: 28193758 Free PMC article. No abstract available.
-
Neurologic involvement in patients with atypical Chediak-Higashi disease.Neurology. 2017 Feb 14;88(7):721. doi: 10.1212/WNL.0000000000003675. Neurology. 2017. PMID: 28193759 Free PMC article. No abstract available.
Retracted and republished in
-
Neurologic involvement in patients with atypical Chediak-Higashi disease.Neurology. 2017 Feb 14;88(7):e57-e65. doi: 10.1212/WNL.0000000000003622. Neurology. 2017. PMID: 28193763 Free PMC article.
Expression of concern in
-
Neurologic involvement in patients with atypical Chediak-Higashi disease.Neurology. 2017 Feb 14;88(7):721. doi: 10.1212/WNL.0000000000003324. Epub 2016 Sep 28. Neurology. 2017. PMID: 27683843 Free PMC article. No abstract available.
Abstract
Objective: To delineate the developmental and progressive neurodegenerative features in 9 young adults with the atypical form of Chediak-Higashi disease (CHD) enrolled in a natural history study.
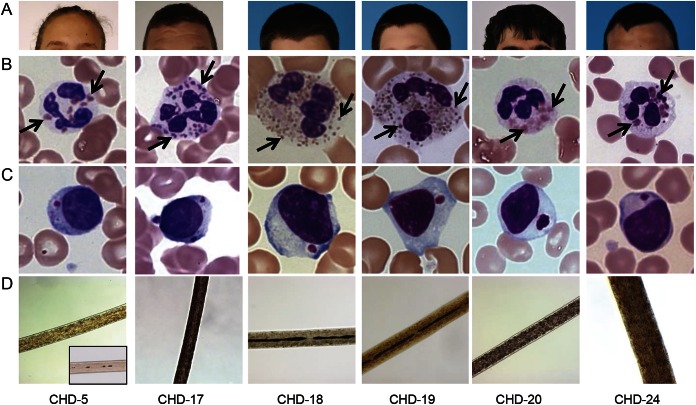
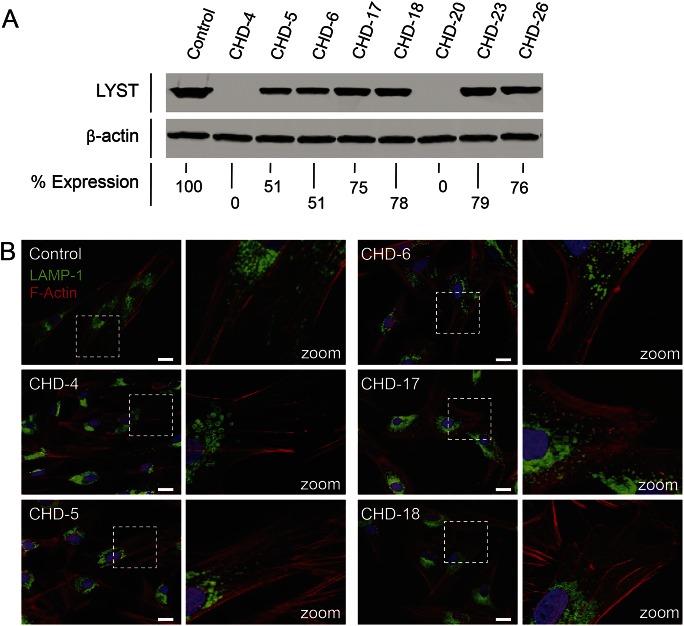
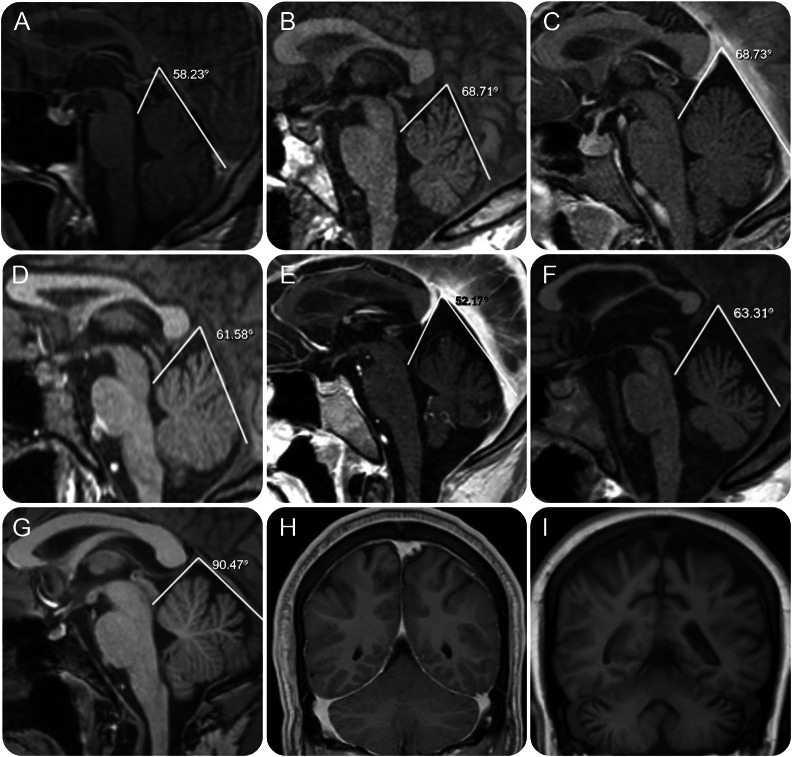
Methods: Patients with atypical clinical features, but diagnostically confirmed CHD by standard evaluation of blood smears and molecular genotyping, underwent complete neurologic evaluation, MRI of the brain, electrophysiologic examination, and neuropsychological testing. Fibroblasts were collected to investigate the cellular phenotype and correlation with the clinical presentation.
Results: In 9 mildly affected patients with CHD, we documented learning and behavioral difficulties along with developmental structural abnormalities of the cerebellum and posterior fossa, which are apparent early in childhood. A range of progressive neurologic problems emerge in early adulthood, including cerebellar deficits, polyneuropathies, spasticity, cognitive decline, and parkinsonism.
Conclusions: Patients with undiagnosed atypical CHD manifesting some of these wide-ranging yet nonspecific neurologic complaints may reside in general and specialty neurology clinics. The absence of the typical bleeding or infectious diathesis in mildly affected patients with CHD renders them difficult to diagnose. Identification of these individuals is important not only for close surveillance of potential CHD-related systemic complications but also for a full understanding of the natural history of CHD and the potential role of the disease-causing protein, LYST, to the pathophysiology of other neurodevelopmental and neurodegenerative disorders.
© 2016 American Academy of Neurology.
Figures
Comment in
-
Findings of research misconduct.NIH Guide Grants Contracts (Bethesda). 2016 Sep 9:NOT-OD-16-145. NIH Guide Grants Contracts (Bethesda). 2016. PMID: 27623616 Free PMC article. No abstract available.
-
Findings of Research Misconduct.Fed Regist. 2016 Aug 30;81(168):59642-59643. Fed Regist. 2016. PMID: 27737275 Free PMC article. No abstract available.
References
-
- Nagle DL, Karim MA, Woolf EA, et al. Identification and mutation analysis of the complete gene for Chediak-Higashi syndrome. Nat Genet 1996;14:307–311. - PubMed
-
- Blume RS, Wolff SM. The Chediak-Higashi syndrome: studies in four patients and a review of the literature. Medicine 1972;51:247–280. - PubMed
-
- Jessen B, Maul-Pavicic A, Ufheil H, et al. Subtle differences in CTL cytotoxicity determine susceptibility to hemophagocytic lymphohistiocytosis in mice and humans with Chediak-Higashi syndrome. Blood 2011;118:4620–4629. - PubMed
-
- Introne W, Boissy RE, Gahl WA. Clinical, molecular, and cell biological aspects of Chediak-Higashi syndrome. Mol Genet Metab 1999;68:283–303. - PubMed
-
- Tardieu M, Lacroix C, Neven B, et al. Progressive neurologic dysfunctions 20 years after allogeneic bone marrow transplantation for Chediak-Higashi syndrome. Blood 2005;106:40–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical