

Cost-effectiveness of Tyrosine Kinase Inhibitor Treatment Strategies for Chronic Myeloid Leukemia in Chronic Phase After Generic Entry of Imatinib in the United States
- PMID: 26944912
- PMCID: PMC4948567
- DOI: 10.1093/jnci/djw003
Cost-effectiveness of Tyrosine Kinase Inhibitor Treatment Strategies for Chronic Myeloid Leukemia in Chronic Phase After Generic Entry of Imatinib in the United States
Abstract
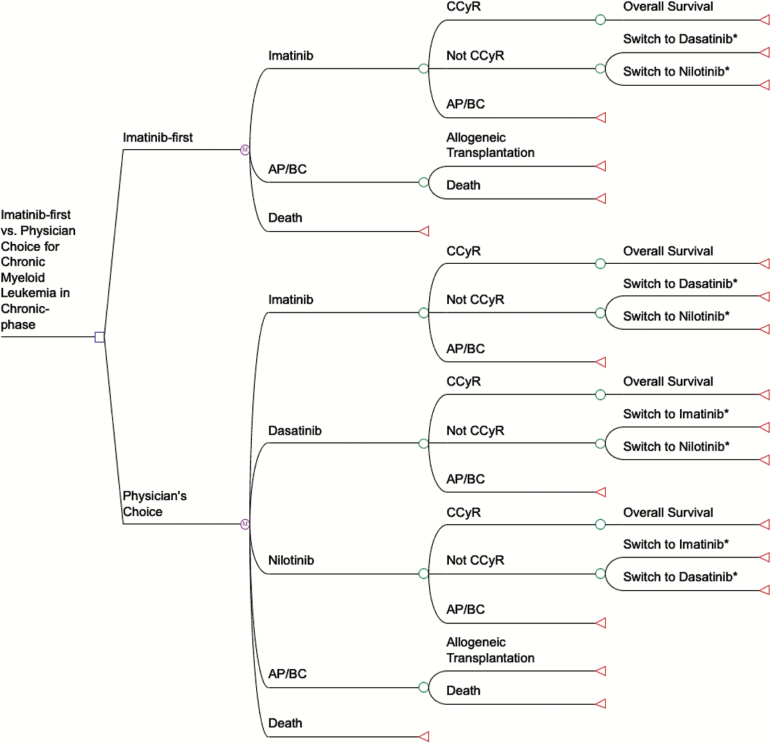
Background: We analyzed the cost-effectiveness of treating incident chronic myeloid leukemia in chronic phase (CML-CP) with generic imatinib when it becomes available in United States in 2016. In the year following generic entry, imatinib's price is expected to drop 70% to 90%. We hypothesized that initiating treatment with generic imatinib in these patients and then switching to the other tyrosine-kinase inhibitors (TKIs), dasatinib or nilotinib, because of intolerance or lack of effectiveness ("imatinib-first") would be cost-effective compared with the current standard of care: "physicians' choice" of initiating treatment with any one of the three TKIs.
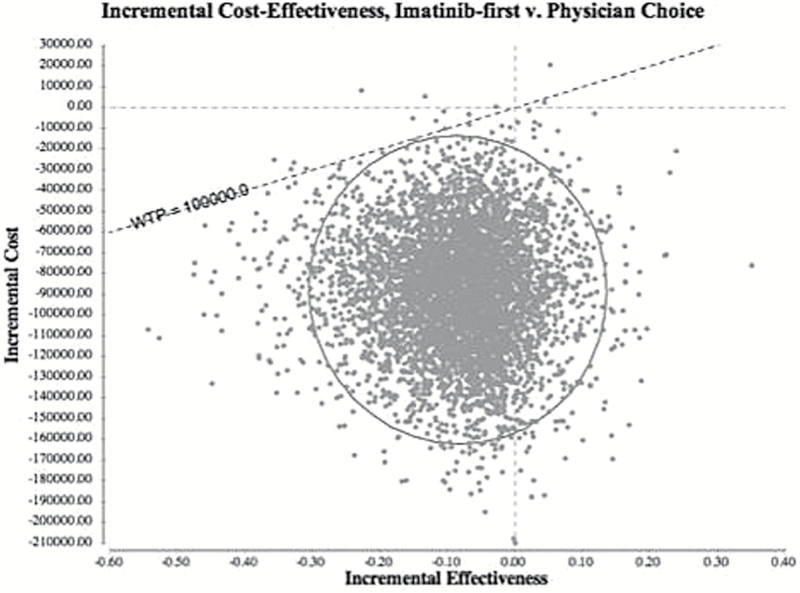
Methods: We constructed Markov models to compare the five-year cost-effectiveness of imatinib-first vs physician's choice from a US commercial payer perspective, assuming 3% annual discounting ($US 2013). The models' clinical endpoint was five-year overall survival taken from a systematic review of clinical trial results. Per-person spending on incident CML-CP treatment overall care components was estimated using Truven's MarketScan claims data. The main outcome of the models was cost per quality-adjusted life-year (QALY). We interpreted outcomes based on a willingness-to-pay threshold of $100 000/QALY. A panel of European LeukemiaNet experts oversaw the study's conduct.
Results: Both strategies met the threshold. Imatinib-first ($277 401, 3.87 QALYs) offered patients a 0.10 decrement in QALYs at a savings of $88 343 over five years to payers compared with physician's choice ($365 744, 3.97 QALYs). The imatinib-first incremental cost-effectiveness ratio was approximately $883 730/QALY. The results were robust to multiple sensitivity analyses.
Conclusion: When imatinib loses patent protection and its price declines, its use will be the cost-effective initial treatment strategy for CML-CP.
© The Author 2016. Published by Oxford University Press.
Figures
Comment in
-
Targeted therapy: Generic imatinib - impact on frontline and salvage therapy for CML.Nat Rev Clin Oncol. 2016 May;13(5):270-2. doi: 10.1038/nrclinonc.2016.59. Nat Rev Clin Oncol. 2016. PMID: 27098218 Free PMC article.
References
-
- O’Brien SG, Guilhot F, Larson RA, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2003;348(11):994–1004. - PubMed
-
- Druker BJ, Guilhot F, O’Brien SG, et al. Five-year follow-up of patients receiving imatinib for chronic myeloid leukemia. N Engl J Med. 2006;355(23):2408–2417. - PubMed
-
- Hughes TP, Kaeda J, Branford S, et al. Frequency of major molecular responses to imatinib or interferon alfa plus cytarabine in newly diagnosed chronic myeloid leukemia. N Engl J Med. 2003;349(15):1423–1432. - PubMed
-
- Deininger M, O’Brien SG, Guilhot F, et al. International Randomized Study of Interferon Vs STI571 (IRIS) 8-Year Follow up: Sustained Survival and Low Risk for Progression or Events in Patients with Newly Diagnosed Chronic Myeloid Leukemia in Chronic Phase (CML-CP) Treated with Imatinib. ASH Annual Meeting Abstracts. 2009;114(22):1126.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
