

Time Is of the Essence: The Impact of Delayed Antibiotic Therapy on Patient Outcomes in Hospital-Onset Enterococcal Bloodstream Infections
- PMID: 26945013
- PMCID: PMC4845789
- DOI: 10.1093/cid/ciw110
Time Is of the Essence: The Impact of Delayed Antibiotic Therapy on Patient Outcomes in Hospital-Onset Enterococcal Bloodstream Infections
Abstract
Background: With increasing prevalence of vancomycin-resistant enterococci (VRE), appropriate antibiotic therapy for enterococcal bloodstream infections (EBSI) can be delayed. Data regarding the impact of delayed therapy on EBSI outcomes are conflicting, and the time delay most strongly associated with poor outcomes has not been defined.
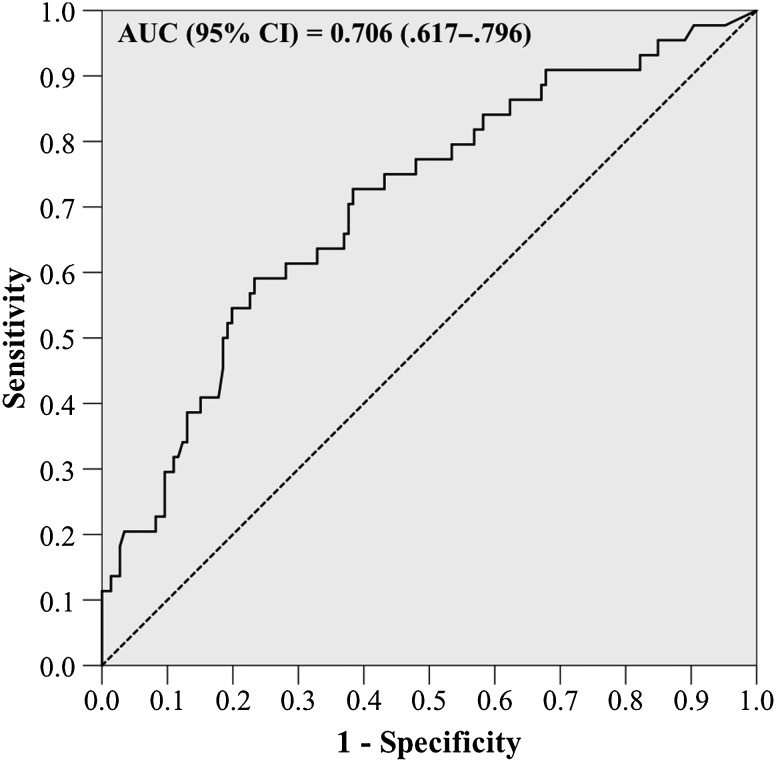
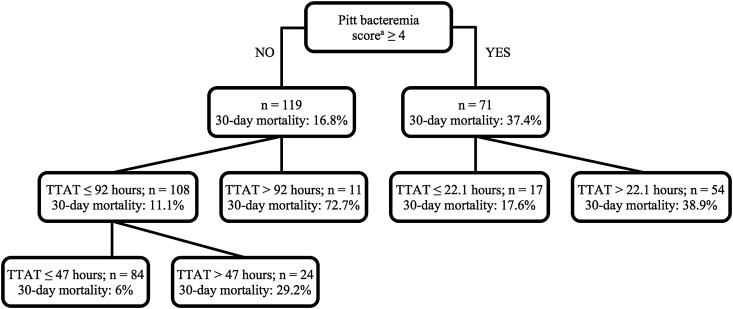
Methods: This was a single-center, retrospective cohort study of adult, nonneutropenic patients with hospital-onset EBSI from 2010 to 2014. Classification and regression tree (CART) analysis was used to determine the delay in appropriate therapy most predictive of 30-day mortality. Appropriate therapy was defined as antibiotic therapy to which the enterococci and copathogen, where applicable, were susceptible. Outcomes and clinical characteristics were compared between patients receiving early or delayed therapy, defined by CART timepoint. Poisson regression was employed to determine the independent association of delayed therapy on 30-day mortality and predictors of delayed therapy.
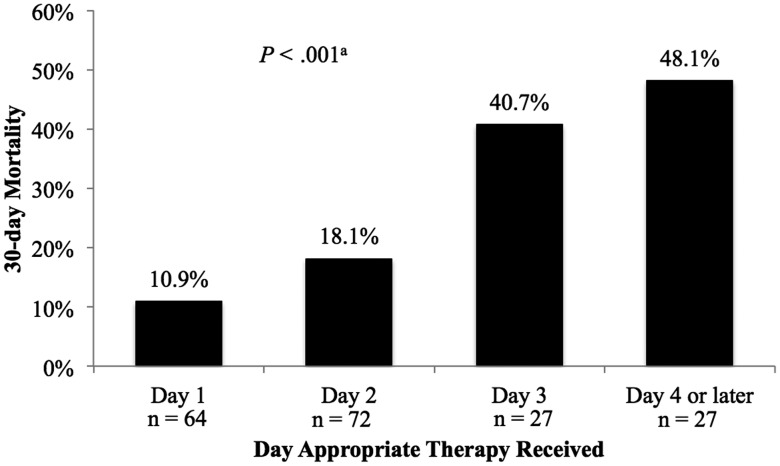
Results: Overall, 190 patients were included. A breakpoint in time to appropriate therapy was identified at 48.1 hours, where 30-day mortality was substantially increased (14.6% vs 45.3%; P < .001). Patients receiving appropriate therapy after 48.1 hours also experienced higher in-hospital mortality and longer EBSI duration. After adjustment for severity of illness and comorbidity, delayed therapy ≥48.1 hours was associated with a 3-fold increase in 30-day mortality (risk ratio, 3.16 [95% confidence interval, 1.96-5.09]). Vancomycin resistance was the only independent predictor of delayed therapy.
Conclusions: In patients with hospital-onset EBSI, receipt of appropriate therapy within the first 48 hours was associated with reduced mortality, underscoring the potential role of rapid diagnostic testing for early identification of VRE.
Keywords: Enterococcus faecalis; Enterococcus faecium; appropriate antibiotic therapy; bacteremia; vancomycin-resistant enterococci.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail journals.permissions@oup.com.
Figures
References
-
- Sievert DM, Ricks P, Edwards JR et al. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2009–2010. Infect Control Hosp Epidemiol 2013; 34:1–14. - PubMed
-
- Osmon DR, Berbari EF, Berendt AR et al. Diagnosis and management of prosthetic joint infection: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 2013; 56:e1–25. - PubMed
-
- Kallen AJ, Mu Y, Bulens S et al. Health care-associated invasive MRSA infections, 2005–2008. JAMA 2010; 304:641–8. - PubMed
-
- Reyes K, Zervos M. Endocarditis caused by resistant Enterococcus: an overview. Curr Infect Dis Rep 2013; 15:320–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
