

A Preoperative Assessment of Significant Coronary Stenosis Based on a Semiquantitative Analysis of Coronary Artery Calcification on Noncontrast Computed Tomography in Aortic Stenosis Patients Undergoing Aortic Valve Replacement
- PMID: 26945385
- PMCID: PMC4782869
- DOI: 10.1097/MD.0000000000002906
A Preoperative Assessment of Significant Coronary Stenosis Based on a Semiquantitative Analysis of Coronary Artery Calcification on Noncontrast Computed Tomography in Aortic Stenosis Patients Undergoing Aortic Valve Replacement
Abstract
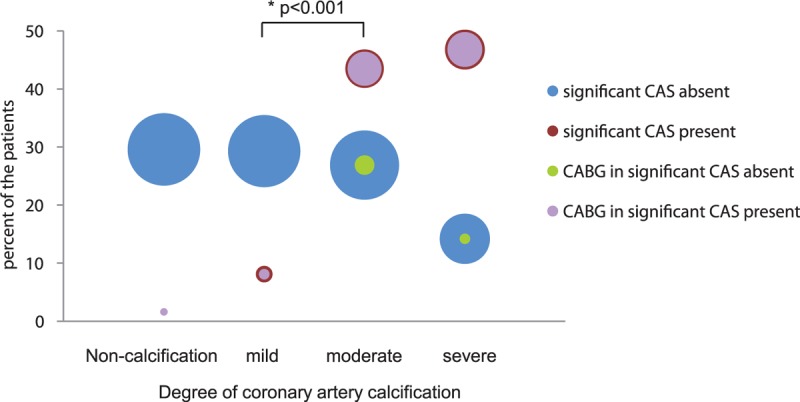
Invasive coronary angiography (ICA) is the recommended assessment for coronary artery disease in patients undergoing elective aortic valve replacement (AVR). Noncontrast computed tomography (CT) is useful for evaluating lung lesions and calcifications at the cannulation site of the ascending aorta. The purpose of this study was to evaluate the role of noncontrast CT in the visual assessment of coronary artery calcification (CAC) in patients undergoing AVR. We retrospectively identified patients with significant aortic stenosis (AS) who were referred for AVR between January 2006 and December 2013. Among these, we included 386 patients (53.6% males, 69.2 ± 8.4 years) who underwent both noncontrast CT and ICA. Significant coronary artery stenosis (CAS) in the ICA was defined as luminal stenosis ≥70%. The 4 main coronary arteries were visually assessed on noncontrast CT and were scored based on the Weston score as follows: 0, no visually detected calcium; 1, a single high-density pixel detected; 3, calcium was dense enough to create a blooming artifact; and 2, calcium in between 1 and 3. Four groups were reclassified by the sum of the Weston scores from each vessel, as follows: noncalcification (0); mild calcification (1-4); moderate calcification (5-8); and severe calcification (9-12). Receiver-operating characteristic (ROC) analysis was generated to identify the cutoff Weston score values for predicting significant CAS. Diagnostic estimates were calculated based on these cutoffs. In the ICA analysis, 62 of the 386 patients (16.1%) had significant CAS. All patients were divided into 4 groups. The noncalcification group had 97 subjects (Weston score 0), the mild degree group had 100 (2.6 ± 1.0), the moderate calcification group had 114 (6.6 ± 1.1), and the severe calcification group had 75 (10.7 ± 1.1). The prevalence of significant CAS in the noncalcification, mild, moderate, and severe groups was 1% (1/97), 5% (5/100), 24% (27/114), and 39% (29/75), respectively. The group with CAS had significantly more CAC than the group without CAS (8.37 ± 2.93 vs 4.01 ± 3.75, P < 0.001). The cutoff value (by Weston score) for predicting significant CAS is ≥5 (sensitivity 90.3%, specificity 59.0%, positive predictive value 29.6%, and negative predictive value 97%). The degree of CAC detected on noncontrast CT can help to predict significant CAS in AS patients who are referred for AVR. For the clinicians, the visual assessment of CAC on noncontrast CT was easy and useful for estimating CAS. Therefore, ICA should be recommended to selective patients based on patients' CAC and Weston scores during the preoperative evaluation for elective AVR.
Conflict of interest statement
The authors report no conflicts of interest.
Figures

Similar articles
-
Aortic root, not valve, calcification correlates with coronary artery calcification in patients with severe aortic stenosis: A two-center study.Atherosclerosis. 2015 Dec;243(2):631-7. doi: 10.1016/j.atherosclerosis.2015.10.014. Epub 2015 Oct 22. Atherosclerosis. 2015. PMID: 26551591
-
Correlation and predictive value of aortic root calcification markers with coronary artery calcification and obstructive coronary artery disease.Radiol Med. 2017 Feb;122(2):113-120. doi: 10.1007/s11547-016-0707-5. Epub 2016 Nov 14. Radiol Med. 2017. PMID: 27844188
-
Third generation dual source CT with ultra-high pitch protocol for TAVI planning and coronary tree assessment: feasibility, image quality and diagnostic performance.Eur J Radiol. 2020 Jan;122:108749. doi: 10.1016/j.ejrad.2019.108749. Epub 2019 Nov 13. Eur J Radiol. 2020. PMID: 31759224
-
Role of preprocedural computed tomography in transcatheter aortic valve implantation.Rofo. 2013 Oct;185(10):941-9. Rofo. 2013. PMID: 24490256 Review.
-
Prognostic value of myocardial computed tomography-derived extracellular volume in severe aortic stenosis requiring aortic valve replacement: a systematic review and meta-analysis.Eur Heart J Cardiovasc Imaging. 2025 Mar 3;26(3):518-531. doi: 10.1093/ehjci/jeae324. Eur Heart J Cardiovasc Imaging. 2025. PMID: 39787608 Free PMC article.
Cited by
-
64-Slice spiral double-low CT to evaluate the degree of stenosis and plaque composition in diagnosing coronary artery disease.Exp Ther Med. 2017 Oct;14(4):3088-3092. doi: 10.3892/etm.2017.4890. Epub 2017 Aug 4. Exp Ther Med. 2017. PMID: 28928803 Free PMC article.
References
-
- Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J 2012; 33:2451–2496. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, et al. American College of Cardiology/American Heart Association Task Force on Practice G. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014; 63:2438–2488. - PubMed
-
- Stefanini GG, Stortecky S, Meier B, et al. Severe aortic stenosis and coronary artery disease. EuroIntervention 2013; 9 (Suppl):S63–S68. - PubMed
-
- Nasir K, Katz R, Al-Mallah M, et al. Relationship of aortic valve calcification with coronary artery calcium severity: the Multi-Ethnic Study of Atherosclerosis (MESA). J Cardiovasc Comput Tomogr 2010; 4:41–46. - PubMed
-
- Silaruks S, Clark D, Thinkhamrop B, et al. Angina pectoris and coronary artery disease in severe isolated valvular aortic stenosis. Heart Lung Circ 2001; 10:14–23. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
