

Inflammation, fracture and bone repair
- PMID: 26946132
- PMCID: PMC4833637
- DOI: 10.1016/j.bone.2016.02.020
Inflammation, fracture and bone repair
Abstract
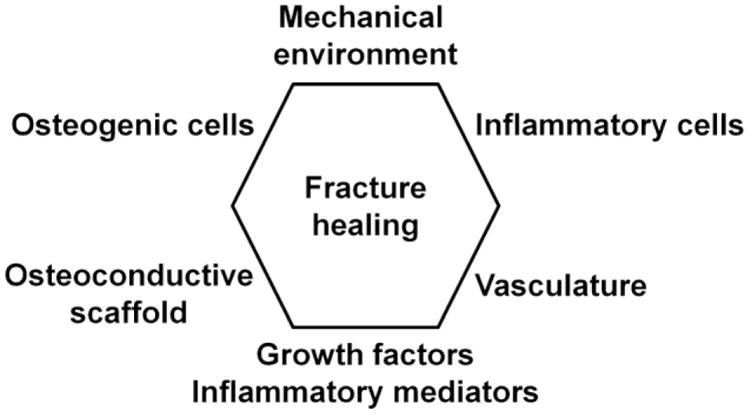
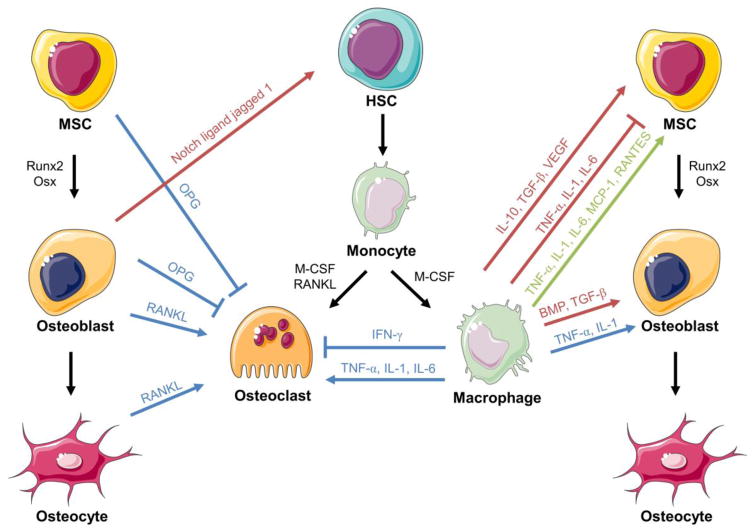
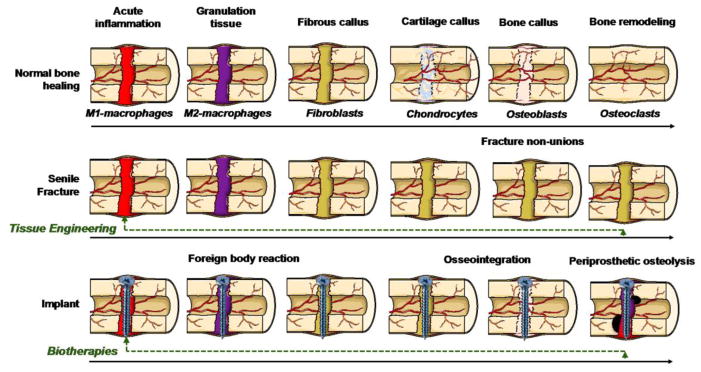
The reconstitution of lost bone is a subject that is germane to many orthopedic conditions including fractures and non-unions, infection, inflammatory arthritis, osteoporosis, osteonecrosis, metabolic bone disease, tumors, and periprosthetic particle-associated osteolysis. In this regard, the processes of acute and chronic inflammation play an integral role. Acute inflammation is initiated by endogenous or exogenous adverse stimuli, and can become chronic in nature if not resolved by normal homeostatic mechanisms. Dysregulated inflammation leads to increased bone resorption and suppressed bone formation. Crosstalk among inflammatory cells (polymorphonuclear leukocytes and cells of the monocyte-macrophage-osteoclast lineage) and cells related to bone healing (cells of the mesenchymal stem cell-osteoblast lineage and vascular lineage) is essential to the formation, repair and remodeling of bone. In this review, the authors provide a comprehensive summary of the literature related to inflammation and bone repair. Special emphasis is placed on the underlying cellular and molecular mechanisms, and potential interventions that can favorably modulate the outcome of clinical conditions that involve bone repair.
Keywords: Bone repair; Fracture healing; Inflammation; Tissue engineering.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Miranda MA, Moon MS. Treatment strategy for nonunions and malunions. In: Stannard JP, Schmidt AH, Kregor PJ, editors. Surgical Treatment of Orthopaedic Trauma. New York: Thieme; 2007. pp. 77–100.
-
- Hak DJ, Fitzpatrick D, Bishop JA, Marsh JL, Tilp S, Schnettler R, Simpson H, Alt V. Delayed union and nonunions: epidemiology, clinical issues, and financial aspects. Injury. 2014;45(Suppl 2):S3–7. - PubMed
-
- National Osteoporosis Foundation. What is Osteoporosis?
-
- Jahangir AA, Nunley RM, Mehta S, Sharan A, Fellows TWHP. Bone-graft substitutes in orthopaedic surgery. AAOS Now. 2008;2:1–5.
-
- Department of Research & Scientific Affairs AAoOS. Annual Incidence of Common Musculoskeletal Procedures and Treatment. 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
