

Factors Associated With Major Adverse Cardiovascular Events After Liver Transplantation Among a National Sample
- PMID: 26946333
- PMCID: PMC5215909
- DOI: 10.1111/ajt.13779
Factors Associated With Major Adverse Cardiovascular Events After Liver Transplantation Among a National Sample
Abstract
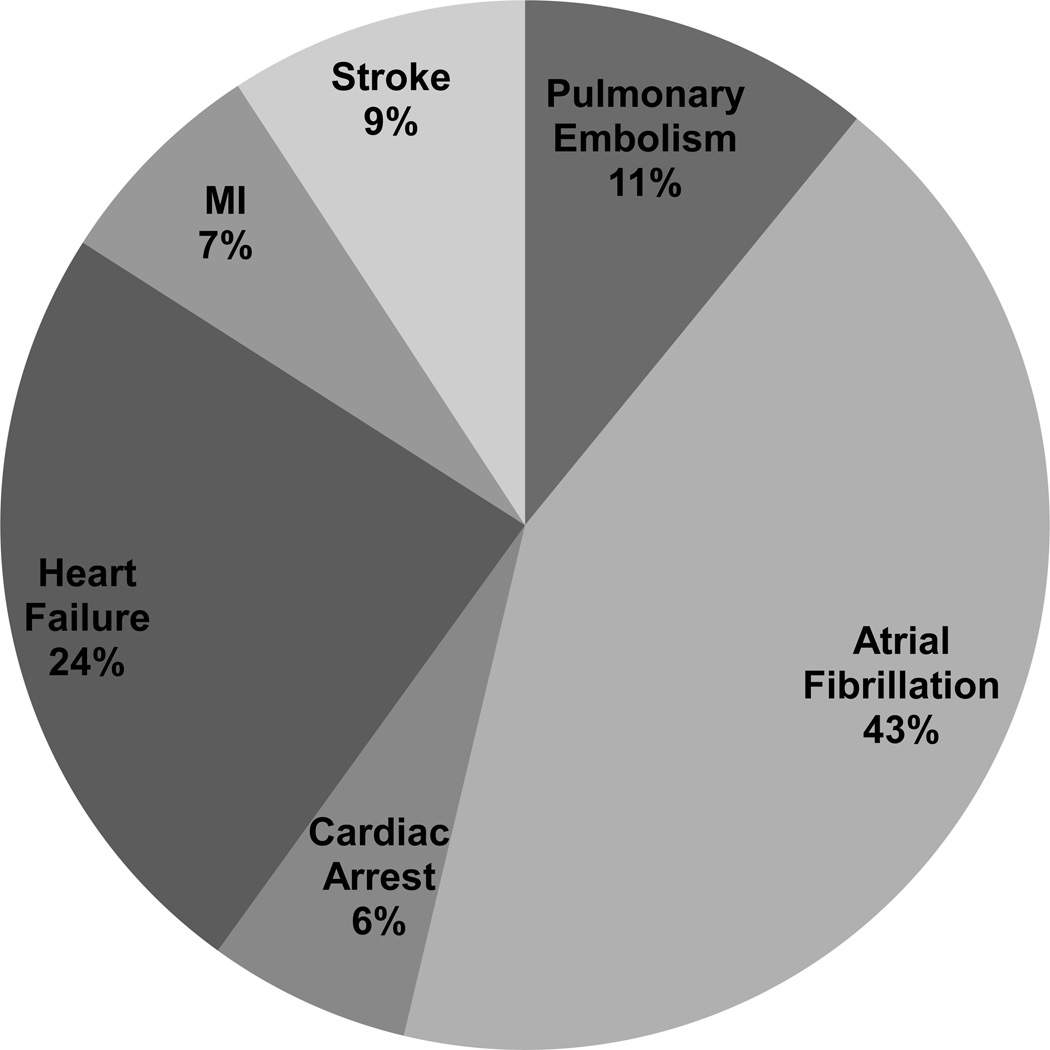
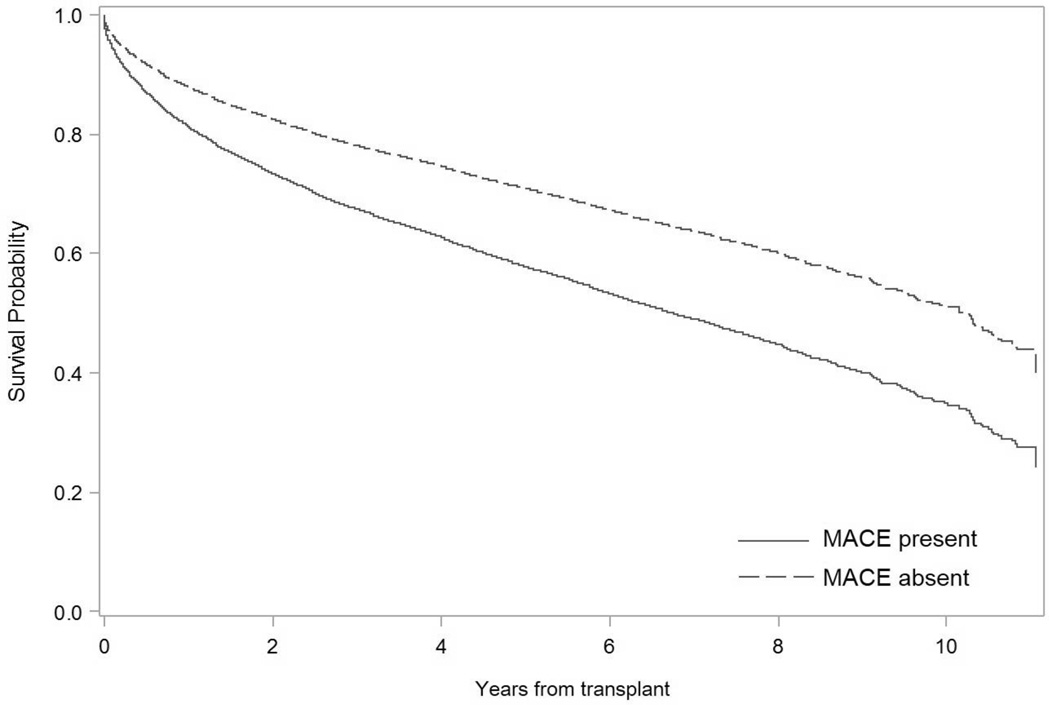
Assessment of major adverse cardiovascular events (MACE) after liver transplantation (LT) has been limited by the lack of a multicenter study with detailed clinical information. An integrated database linking information from the University HealthSystem Consortium and the Organ Procurement and Transplant Network was analyzed using multivariate Poisson regression to assess factors associated with 30- and 90-day MACE after LT (February 2002 to December 2012). MACE was defined as myocardial infarction (MI), heart failure (HF), atrial fibrillation (AF), cardiac arrest, pulmonary embolism, and/or stroke. Of 32 810 recipients, MACE hospitalizations occurred in 8% and 11% of patients at 30 and 90 days, respectively. Recipients with MACE were older and more likely to have a history of nonalcoholic steatohepatitis (NASH), alcoholic cirrhosis, MI, HF, stroke, AF and pulmonary and chronic renal disease than those without MACE. In multivariable analysis, age >65 years (incidence rate ratio [IRR] 2.8, 95% confidence interval [95% CI] 1.8-4.4), alcoholic cirrhosis (IRR 1.6, 95% CI 1.2-2.2), NASH (IRR 1.6, 95% CI 1.1-2.4), pre-LT creatinine (IRR 1.1, 95% CI 1.04-1.2), baseline AF (IRR 6.9, 95% CI 5.0-9.6) and stroke (IRR 6.3, 95% CI 1.6-25.4) were independently associated with MACE. MACE was associated with lower 1-year survival after LT (79% vs. 88%, p < 0.0001). In a national database, MACE occurred in 11% of LT recipients and had a negative impact on survival. Pre-LT AF and stroke substantially increase the risk of MACE, highlighting potentially high-risk LT candidates.
Keywords: Organ Procurement and Transplantation Network (OPTN); cardiovascular disease; clinical research/practice; comorbidities; complication: medical/metabolic; health services and outcomes research; liver transplantation/hepatology; risk assessment/risk stratification.
© Copyright 2016 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose.
Figures
References
-
- Albeldawi M, Aggarwal A, Madhwal S, Cywinski J, Lopez R, Eghtesad B, et al. Cumulative risk of cardiovascular events after orthotopic liver transplantation. Liver Transpl. 2012;18(3):370–375. - PubMed
-
- Johnston SD, Morris JK, Cramb R, Gunson BK, Neuberger J. Cardiovascular morbidity and mortality after orthotopic liver transplantation. Transplantation. 2002;73(6):901–906. - PubMed
-
- Annual Report of the U.S. Organ Procurement and Transplantation Network (OPTN) and the Scientific Registry of Transplant Recipients (SRTR): Transplant Data 1998–2011. Rockville, MD: Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation; 2012.
-
- Audet M, Piardi T, Panaro F, Cag M, Ghislotti E, Habibeh H, et al. Liver transplantation in recipients over 65 yr old: a single center experience. Clin Transplant. 2010;24(1):84–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
