

Health Behaviors, Mental Health, and Health Care Utilization Among Single Mothers After Welfare Reforms in the 1990s
- PMID: 26946395
- PMCID: PMC5013929
- DOI: 10.1093/aje/kwv249
Health Behaviors, Mental Health, and Health Care Utilization Among Single Mothers After Welfare Reforms in the 1990s
Abstract
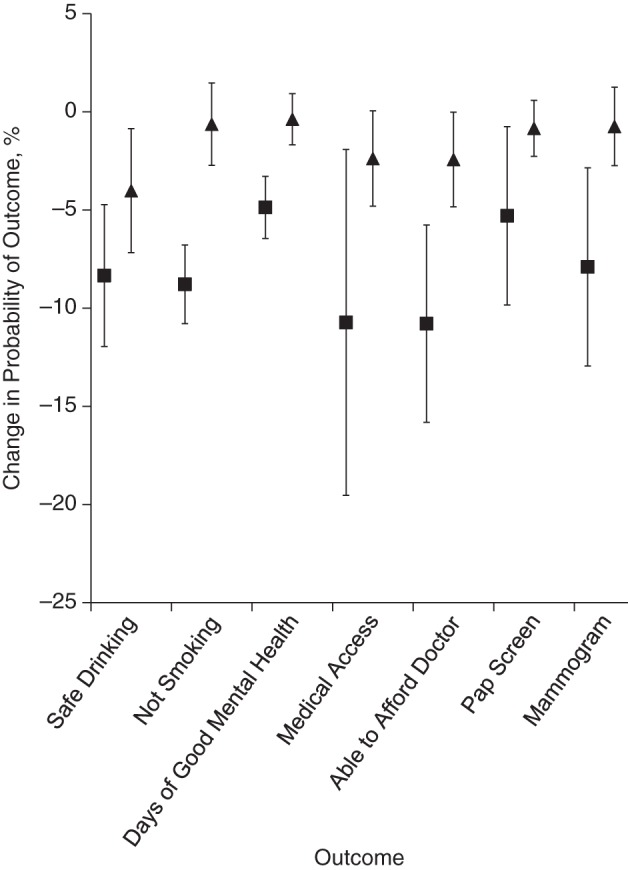
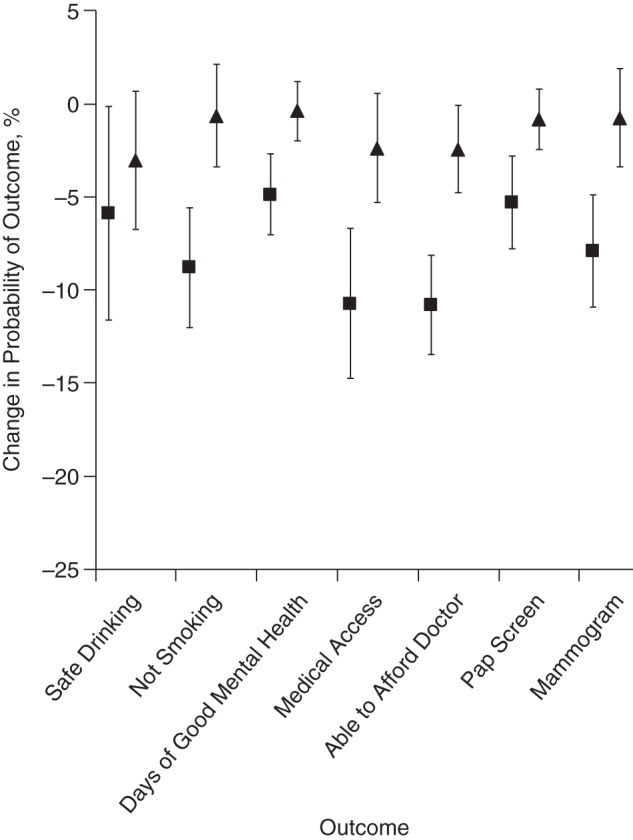
We studied the health of low-income US women affected by the largest social policy change in recent US history: the 1996 welfare reforms. Using the Behavioral Risk Factor Surveillance System (1993-2012), we performed 2 types of analysis. First, we used difference-in-difference-in-differences analyses to estimate associations between welfare reforms and health outcomes among the most affected women (single mothers aged 18-64 years in 1997; n = 219,469) compared with less affected women (married mothers, single nonmothers, and married nonmothers of the same age range in 1997; n = 2,422,265). We also used a synthetic control approach in which we constructed a more ideal control group for single mothers by weighting outcomes among the less affected groups to match pre-reform outcomes among single mothers. In both specifications, the group most affected by welfare reforms (single mothers) experienced worse health outcomes than comparison groups less affected by the reforms. For example, the reforms were associated with at least a 4.0-percentage-point increase in binge drinking (95% confidence interval: 0.9, 7.0) and a 2.4-percentage-point decrease in the probability of being able to afford medical care (95% confidence interval: 0.1, 4.8) after controlling for age, educational level, and health care insurance status. Although the reforms were applauded for reducing welfare dependency, they may have adversely affected health.
Keywords: health behaviors; health care utilization; self-rated health; single mothers; welfare reform.
© The Author 2016. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Invited Commentary: An Interdisciplinary Approach for Policy Evaluation.Am J Epidemiol. 2016 Mar 15;183(6):539-41. doi: 10.1093/aje/kwv237. Epub 2016 Mar 5. Am J Epidemiol. 2016. PMID: 26946396 Free PMC article.
-
Basu et al. Respond to "Interdisciplinary Approach for Policy Evaluation".Am J Epidemiol. 2016 Mar 15;183(6):542-3. doi: 10.1093/aje/kwv239. Epub 2016 Mar 5. Am J Epidemiol. 2016. PMID: 26946397 Free PMC article. No abstract available.
References
-
- Piketty T, Saez E. Inequality in the long run. Science. 2014;3446186:838–843. - PubMed
-
- Olshansky SJ, Passaro DJ, Hershow RC et al. . A potential decline in life expectancy in the United States in the 21st century. N Engl J Med. 2005;35211:1138–1145. - PubMed
-
- Cohen B, Preston SH, Crimmins EM et al. . Explaining Divergent Levels of Longevity in High-Income Countries. Washington, DC: National Academies Press; 2011. - PubMed
-
- Solow RM. Work and Welfare. Princeton, NJ: Princeton University Press; 2009.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
