

Cost-benefit analysis of the polypill in the primary prevention of myocardial infarction and stroke
- PMID: 26946426
- PMCID: PMC4877433
- DOI: 10.1007/s10654-016-0122-1
Cost-benefit analysis of the polypill in the primary prevention of myocardial infarction and stroke
Abstract
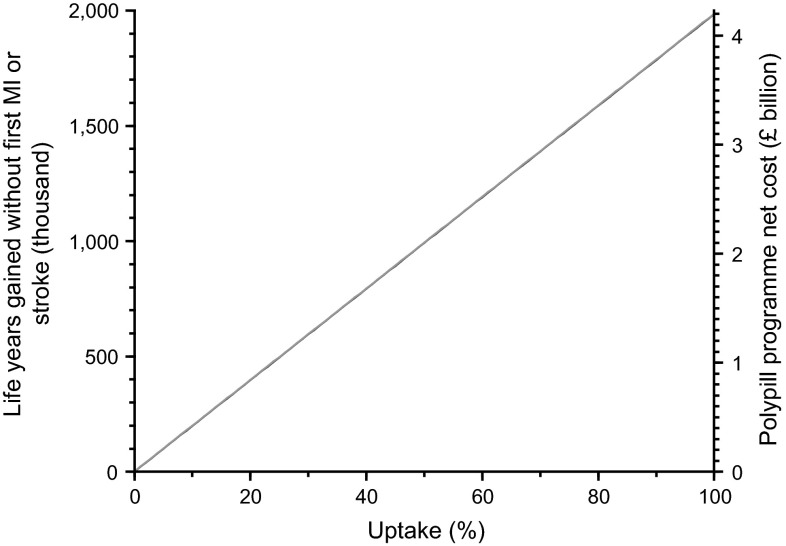
The primary prevention of cardiovascular disease is a public health priority. To assess the costs and benefits of a Polypill Prevention Programme using a daily 4-component polypill from age 50 in the UK, we determined the life years gained without a first myocardial infarction (MI) or stroke, together with the total service cost (or saving) and the net cost (or saving) per year of life gained without a first MI or stroke. This was estimated on the basis of a 50 % uptake and a previously published 83 % treatment adherence. The total years of life gained without a first MI or stroke in a mature programme is 990,000 each year in the UK. If the cost of the Polypill Prevention Programme were £1 per person per day, the total cost would be £4.76 bn and, given the savings (at 2014 prices) of £2.65 bn arising from the disease prevented, there would be a net cost of £2.11 bn representing a net cost per year of life gained without a first MI or stroke of £2120. The results are robust to sensitivity analyses. A national Polypill Prevention Programme would have a substantial effect in preventing MIs and strokes and be cost-effective.
Keywords: Cardiovascular diseases; Cost–benefit analysis; Myocardial infarction; Polypill; Primary prevention; Stroke.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
