

Early goal-directed resuscitation for patients with severe sepsis and septic shock: a meta-analysis and trial sequential analysis
- PMID: 26946514
- PMCID: PMC4779580
- DOI: 10.1186/s13049-016-0214-7
Early goal-directed resuscitation for patients with severe sepsis and septic shock: a meta-analysis and trial sequential analysis
Abstract
Background: The aim of this study was to explore whether early goal-directed therapy (EGDT) was associated with a lower mortality rate in comparison to usual care in patients with severe sepsis and septic shock.
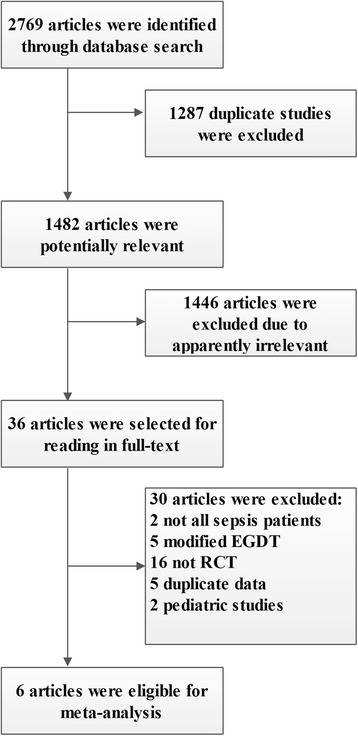
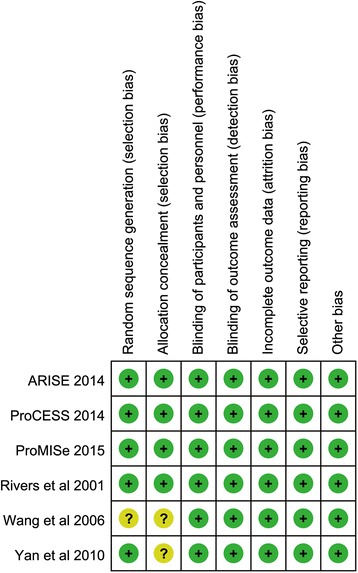
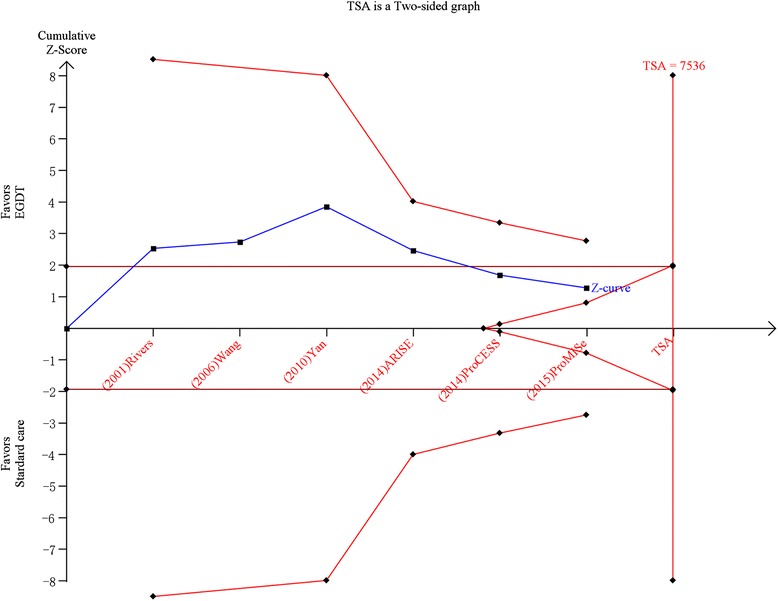
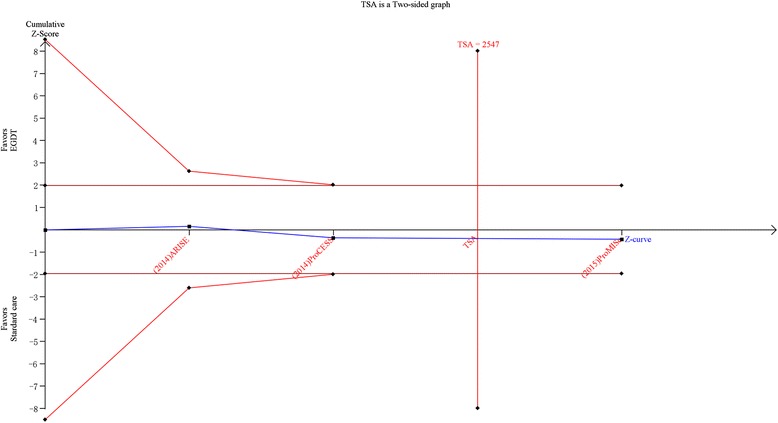
Methods: PubMed, EMBASE, Cochrane library and a Chinese database (SinoMed) were searched systematically to identify randomized controlled trials (RCTs) comparing standard EGDT with usual care in resuscitation of patients with severe sepsis and septic shock and the search time could date back to the publication of the study by Rivers in 2001. The study selection, data extraction and methodological evaluation were performed by two investigators independently. The primary outcome was all-cause mortality. The present meta-analysis had been registered in PROSPERO (CRD42015017667).
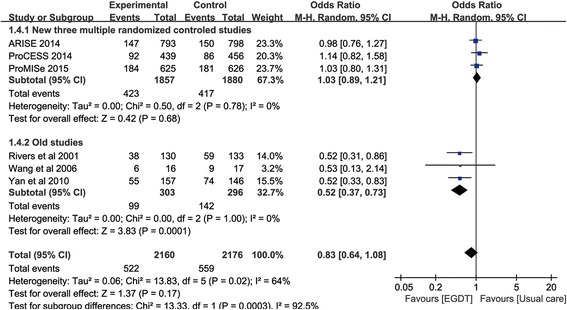
Results: Our meta-analysis identified 6 studies and enrolling 4336 patients. There was no significant difference in mortality between the two groups, and the pooled odds ratio (OR) was 0.83 (95 % confident interval, CI, 0.64-1.08) with significant heterogeneity (p = 0.02, I(2) = 64%). However, the pooled OR of 3 multicenter RCTs was 1.03 (95% CI, 0.89-1.21) with no heterogeneity (p = 0.78, I(2) = 0%). The effects of EGDT on length of stay in the emergency department and intensive care unit were uncertain, and there was no effect of EGDT on hospital length of stay. There were no differences of mechanical ventilation rate and renal replacement therapy rate between the two groups, and patients in the EGDT group were more admitted in ICU than patients in the control group. During the early 6-h intervention period, patients in the EGDT group received more intravenous fluids, had a higher vasopressor usage rate, higher dobutamine usage rate and higher blood transfusion rate, than patients in the control group. Finally, there was no difference in the incidence of adverse events between the two groups, and the pooled OR was 1.06 (95%CI 0.80-1.39) with moderate heterogeneity (I(2) = 62%, p = 0.07).
Discussion: Our meta-analysis showed that the application of EGDT was not associated with lower mortality rate currently. However it does not mean that it is useless of EGDT in patients with sever sepsis and septic shock. On the contrary, there was no difference in mortality rate between the two groups may be due to the improvement of therapeutic strategies in these patients. And the results may be related to the different compliance rate of EGDT resuscitation bundle.
Conclusions: The current evidence does not support the significant advantage of Early goal-directed therapy (EGDT) in the resuscitation of patients with severe sepsis and septic shock.
Figures
Similar articles
-
Early goal-directed and lactate-guided therapy in adult patients with severe sepsis and septic shock: a meta-analysis of randomized controlled trials.J Transl Med. 2018 Nov 29;16(1):331. doi: 10.1186/s12967-018-1700-7. J Transl Med. 2018. PMID: 30486885 Free PMC article.
-
Early goal-directed therapy in the management of severe sepsis or septic shock in adults: a meta-analysis of randomized controlled trials.BMC Med. 2015 Apr 3;13:71. doi: 10.1186/s12916-015-0312-9. BMC Med. 2015. PMID: 25885654 Free PMC article.
-
Early Goal-Directed Therapy in Severe Sepsis and Septic Shock: A Meta-Analysis and Trial Sequential Analysis of Randomized Controlled Trials.J Intensive Care Med. 2018 May;33(5):296-309. doi: 10.1177/0885066616671710. Epub 2016 Oct 22. J Intensive Care Med. 2018. PMID: 27756870
-
The effect of early goal-directed therapy on mortality in patients with severe sepsis and septic shock: a meta-analysis.J Surg Res. 2016 May 15;202(2):389-97. doi: 10.1016/j.jss.2015.12.048. Epub 2016 Jan 4. J Surg Res. 2016. PMID: 27229114
-
The Effect of Early Goal-Directed Therapy on Outcome in Adult Severe Sepsis and Septic Shock Patients: A Meta-Analysis of Randomized Clinical Trials.Anesth Analg. 2016 Aug;123(2):371-81. doi: 10.1213/ANE.0000000000001278. Anesth Analg. 2016. PMID: 27049857 Free PMC article. Review.
Cited by
-
Impact of Point-of-Care Ultrasound in the Emergency Department on Care Processes and Outcomes in Critically Ill Nontraumatic Patients.Crit Care Explor. 2019 Jun 26;1(6):e0019. doi: 10.1097/CCE.0000000000000019. eCollection 2019 Jun. Crit Care Explor. 2019. PMID: 32166263 Free PMC article.
-
Significance of hydrogen sulfide in sepsis-induced myocardial injury in rats.Exp Ther Med. 2017 Sep;14(3):2153-2161. doi: 10.3892/etm.2017.4742. Epub 2017 Jul 9. Exp Ther Med. 2017. PMID: 28962136 Free PMC article.
-
Hypoalbuminemia, Low Base Excess Values, and Tachypnea Predict 28-Day Mortality in Severe Sepsis and Septic Shock Patients in the Emergency Department.Yonsei Med J. 2016 Nov;57(6):1361-9. doi: 10.3349/ymj.2016.57.6.1361. Yonsei Med J. 2016. PMID: 27593863 Free PMC article. Clinical Trial.
-
Early goal-directed and lactate-guided therapy in adult patients with severe sepsis and septic shock: a meta-analysis of randomized controlled trials.J Transl Med. 2018 Nov 29;16(1):331. doi: 10.1186/s12967-018-1700-7. J Transl Med. 2018. PMID: 30486885 Free PMC article.
-
Early management of sepsis with emphasis on early goal directed therapy: AME evidence series 002.J Thorac Dis. 2017 Feb;9(2):392-405. doi: 10.21037/jtd.2017.02.10. J Thorac Dis. 2017. PMID: 28275488 Free PMC article. Review.
References
-
- The Australasian Resuscitation in Sepsis Evaluation (ARISE) Investigators, Australian and New Zealand Intensive Care Society (ANZICS) Adult Patient Database (APD) Management Committee The outcome of sepsis and septic shock presenting to the emergency departments of Australia and New Zealand. Crit Care Resusc. 2007;9:8–18. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
