

Discovery of a Biological Mechanism of Active Transport through the Tympanic Membrane to the Middle Ear
- PMID: 26946957
- PMCID: PMC4780071
- DOI: 10.1038/srep22663
Discovery of a Biological Mechanism of Active Transport through the Tympanic Membrane to the Middle Ear
Abstract
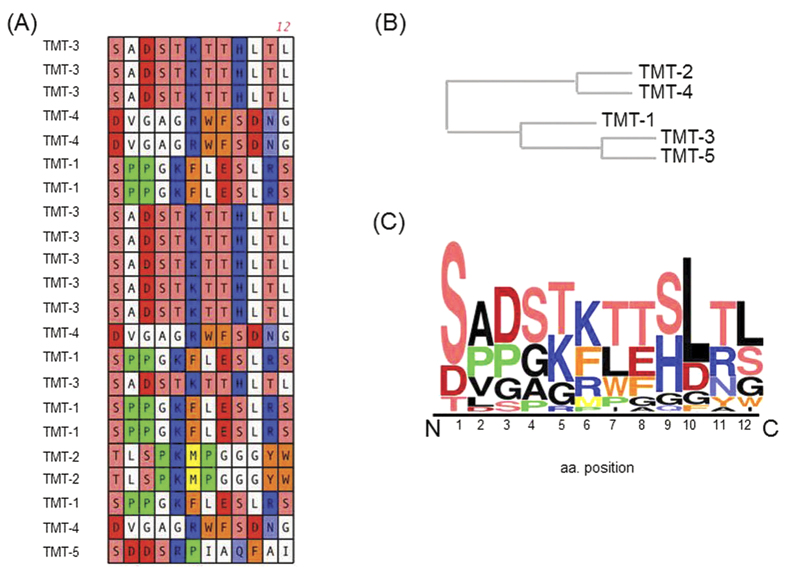
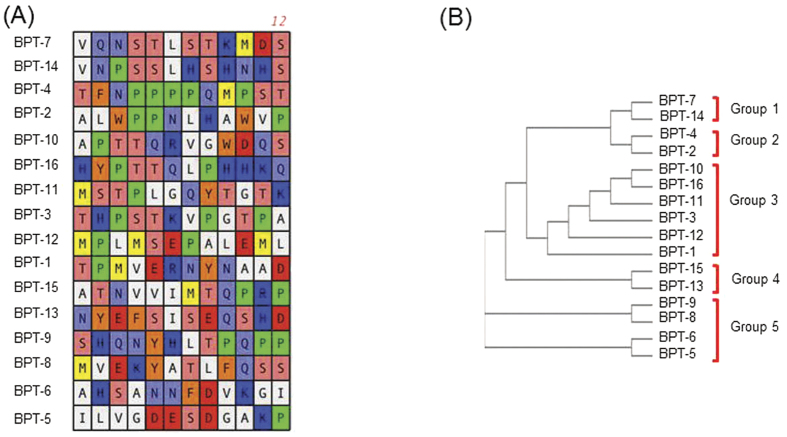
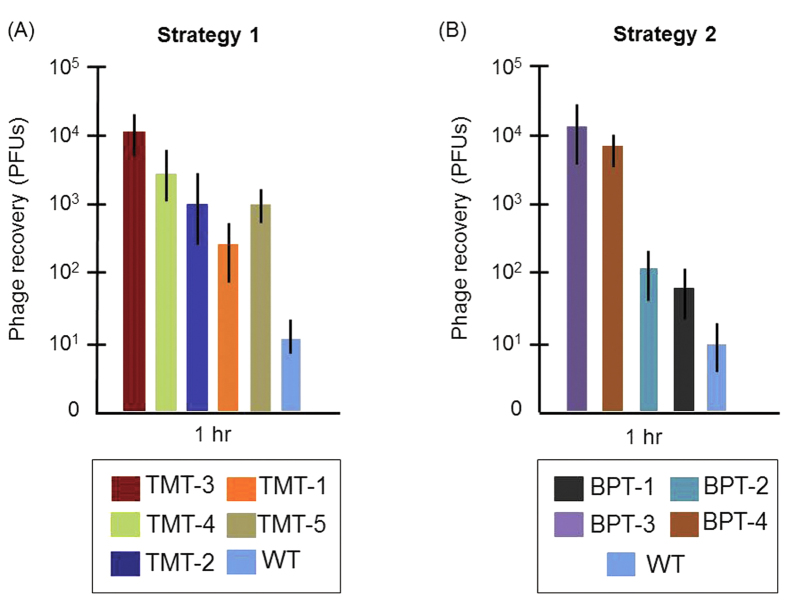
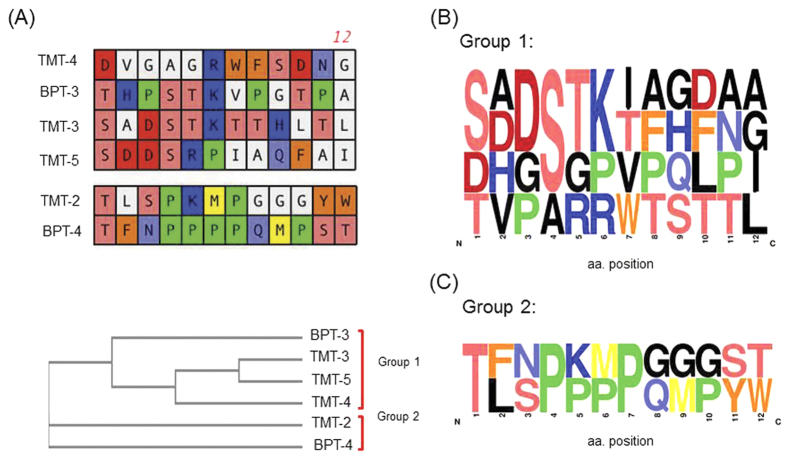
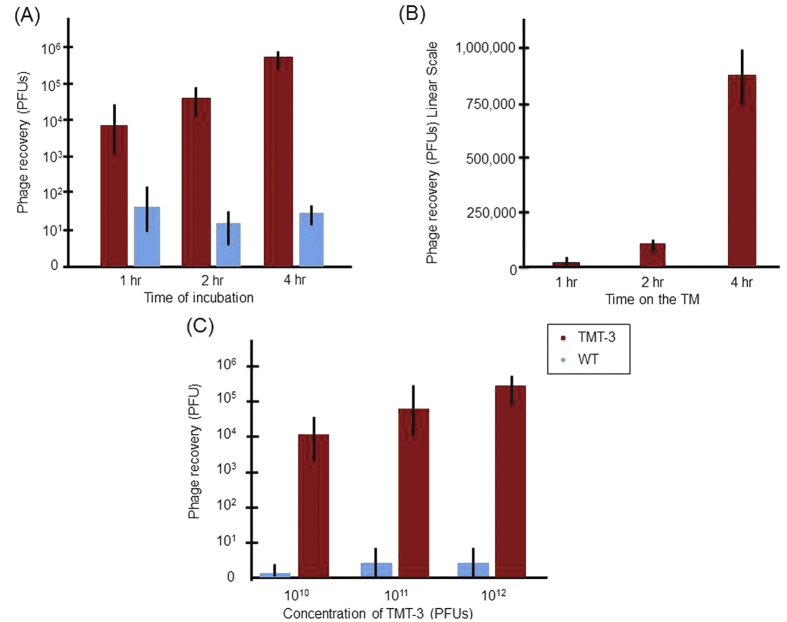
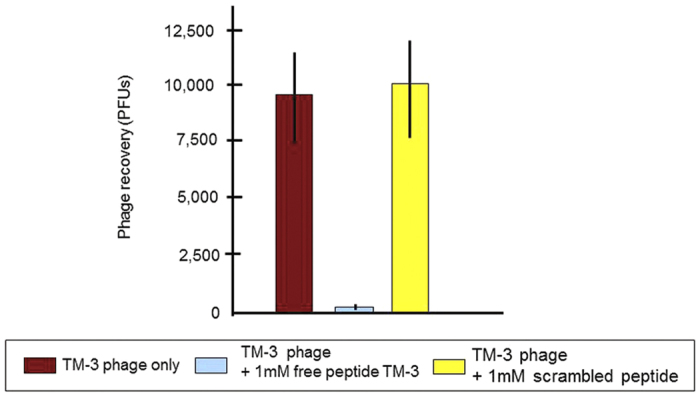
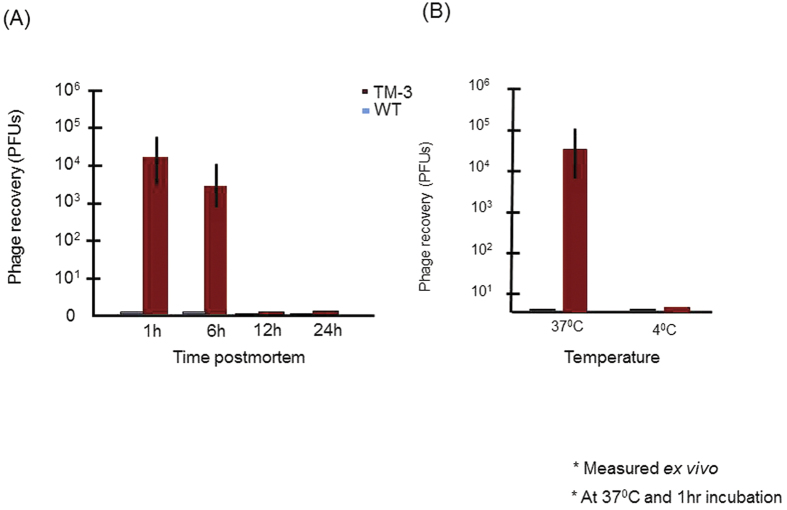
Otitis media (OM) is a common pediatric disease for which systemic antibiotics are often prescribed. While local treatment would avoid the systemic treatment side-effects, the tympanic membrane (TM) represents an impenetrable barrier unless surgically breached. We hypothesized that the TM might harbor innate biological mechanisms that could mediate trans-TM transport. We used two M13-bacteriophage display biopanning strategies to search for mediators of trans-TM transport. First, aliquots of linear phage library displaying 10(10th) 12mer peptides were applied on the TM of rats with active bacterial OM. The middle ear (ME) contents were then harvested, amplified and the preparation re-applied for additional rounds. Second, the same naïve library was sequentially screened for phage exhibiting TM binding, internalization and then transit. Results revealed a novel set of peptides that transit across the TM to the ME in a time and temperature dependent manner. The peptides with highest transport capacities shared sequence similarities. Historically, the TM was viewed as an impermeable barrier. However, our studies reveal that it is possible to translocate peptide-linked small particles across the TM. This is the first comprehensive biopanning for the isolation of TM transiting peptidic ligands. The identified mechanism offers a new drug delivery platform into the ME.
Figures
Similar articles
-
Peptides actively transported across the tympanic membrane: Functional and structural properties.PLoS One. 2017 Feb 24;12(2):e0172158. doi: 10.1371/journal.pone.0172158. eCollection 2017. PLoS One. 2017. PMID: 28234923 Free PMC article.
-
Peptides rapidly transport antibiotic across the intact tympanic membrane to treat a middle ear infection.Drug Deliv. 2025 Dec;32(1):2463427. doi: 10.1080/10717544.2025.2463427. Epub 2025 Feb 17. Drug Deliv. 2025. PMID: 39960246 Free PMC article.
-
Optimisation of peptides that actively cross the tympanic membrane by random amino acid extension: a phage display study.J Drug Target. 2018 Feb;26(2):127-134. doi: 10.1080/1061186X.2017.1347791. Epub 2017 Aug 16. J Drug Target. 2018. PMID: 28658990 Free PMC article.
-
Panel 1: Biotechnology, biomedical engineering and new models of otitis media.Int J Pediatr Otorhinolaryngol. 2020 Mar;130 Suppl 1(Suppl 1):109833. doi: 10.1016/j.ijporl.2019.109833. Epub 2019 Dec 27. Int J Pediatr Otorhinolaryngol. 2020. PMID: 31901291 Free PMC article. Review.
-
Optical Coherence Tomography of the Tympanic Membrane and Middle Ear: A Review.Otolaryngol Head Neck Surg. 2018 Sep;159(3):424-438. doi: 10.1177/0194599818775711. Epub 2018 May 22. Otolaryngol Head Neck Surg. 2018. PMID: 29787354 Review.
Cited by
-
Ayurvedic Management of Presbycusis (Project TOPMAC): Protocol for an Exploratory Randomized Controlled Trial.JMIR Res Protoc. 2024 Sep 23;13:e55089. doi: 10.2196/55089. JMIR Res Protoc. 2024. PMID: 39312772 Free PMC article.
-
Getting Drugs Across Biological Barriers.Adv Mater. 2017 Oct;29(37):10.1002/adma.201606596. doi: 10.1002/adma.201606596. Epub 2017 Jul 28. Adv Mater. 2017. PMID: 28752600 Free PMC article. Review.
-
Drug Delivery across Barriers to the Middle and Inner Ear.Adv Funct Mater. 2021 Oct 26;31(44):2008701. doi: 10.1002/adfm.202008701. Epub 2020 Dec 4. Adv Funct Mater. 2021. PMID: 34795553 Free PMC article.
-
Peptides actively transported across the tympanic membrane: Functional and structural properties.PLoS One. 2017 Feb 24;12(2):e0172158. doi: 10.1371/journal.pone.0172158. eCollection 2017. PLoS One. 2017. PMID: 28234923 Free PMC article.
-
Peptides rapidly transport antibiotic across the intact tympanic membrane to treat a middle ear infection.Drug Deliv. 2025 Dec;32(1):2463427. doi: 10.1080/10717544.2025.2463427. Epub 2025 Feb 17. Drug Deliv. 2025. PMID: 39960246 Free PMC article.
References
-
- Thomas N. M. & Brook I. Otitis media: an update on current pharmacotherapy and future perspectives. Expert Opin Pharmacother. 15, 1069–1083 (2014). - PubMed
-
- Lieberthal A. S. et al.. The Diagnosis and Management of Acute Otitis Media. Pediatrics. 131, e964–e999 (2013). - PubMed
-
- Rosenfeld R. M. et al.. Clinical practice guideline: Tympanostomy tubes in children. Otolaryngol-Head Neck Surg. 149, S1–S35 (2013). - PubMed
-
- Acuin J. Chronic suppurative otitis media: burden of illness and management options Geneva, Switzerland: World Health Organization. (2004) Available at: http://www.who.int/pbd/publications/ Chronicsuppurativeotitis_media.pdf. (Accessed: 26 July 2015).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
