

Psoriasiform eruptions during Kawasaki disease (KD): A distinct phenotype
- PMID: 26946987
- PMCID: PMC4912865
- DOI: 10.1016/j.jaad.2016.02.1146
Psoriasiform eruptions during Kawasaki disease (KD): A distinct phenotype
Abstract
Background: A psoriasis-like eruption develops in a subset of patients with Kawasaki disease (KD).
Objective: We sought to systematically compare KD-associated psoriasiform eruptions with classic psoriasis and the outcomes of KD in children with and without this rash.
Methods: This was a retrospective study of 11 KD cases with a psoriasiform eruption matched 1:2 by age, gender, and ethnicity with psoriasis-only and KD-only controls. Genotyping was performed in 10 cases for a deletion of 2 late cornified envelope (LCE) genes, LCE3C_LCE3B-del, associated with increased risk for pediatric-onset psoriasis.
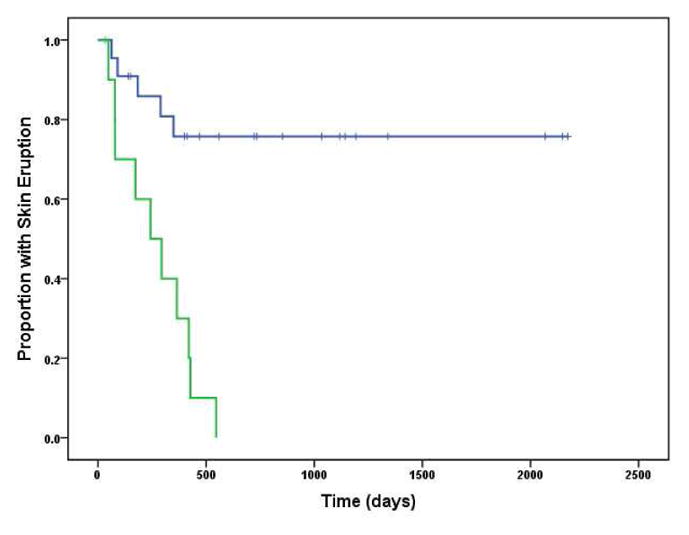
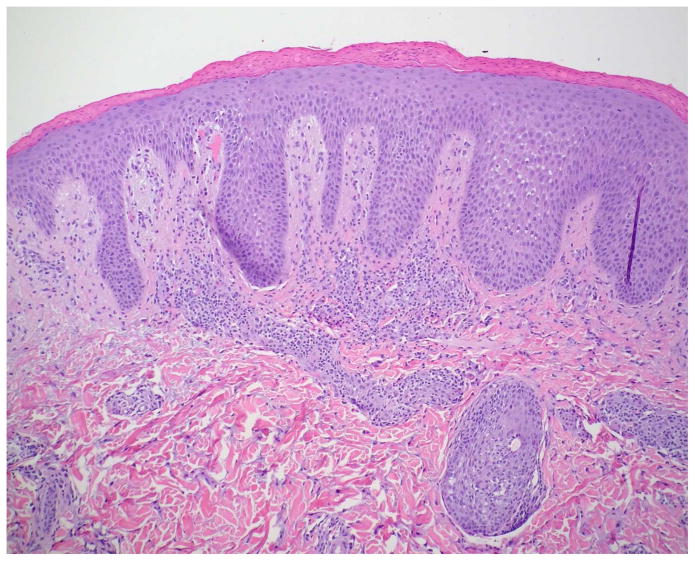
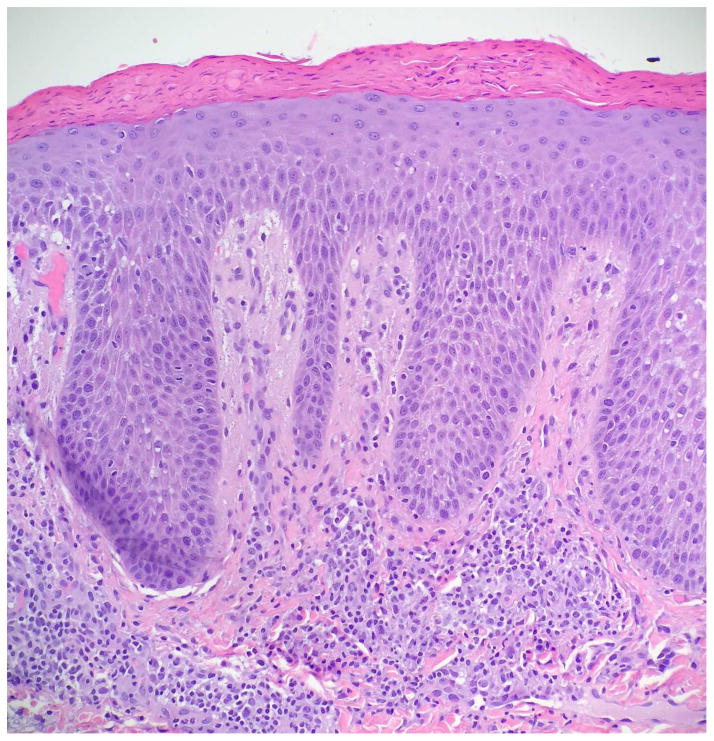
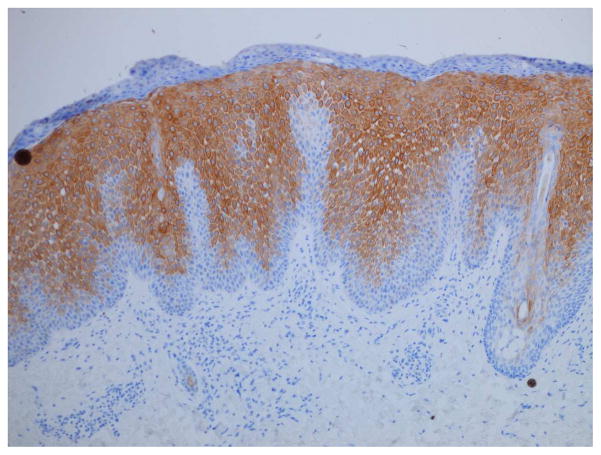
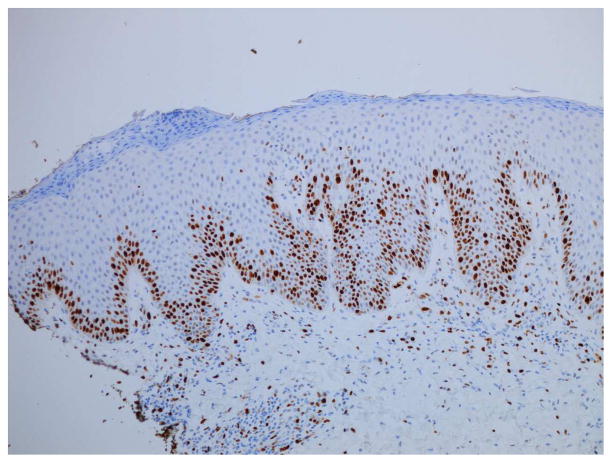
Results: Similar to classic psoriasis, KD-associated eruptions were characterized clinically by well-demarcated, scaly pink plaques and histopathologically by intraepidermal neutrophils, suprabasilar keratin 16 expression, and increased Ki-67 expression. They showed less frequent diaper area involvement, more crust and serous exudate, and an enduring remission (91% vs 23% with confirmed resolution; P < .001). Frequency of LCE3C_LCE3B-del and major KD outcomes were similar between cases and controls.
Limitations: The study was limited by the small number of cases, treatment variation, and availability of skin biopsy specimens.
Conclusions: Although the overall clinical and histopathologic findings were similar to conventional psoriasis, this appears to be a distinct phenotype with significantly greater propensity for remission. No adverse effect on KD outcomes was noted.
Keywords: Kawasaki disease; Ki-67; LCE3C_LCE3B deletion; keratin 16; psoriasiform; psoriasis.
Copyright © 2016 American Academy of Dermatology, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures




References
-
- Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110:2747–2771. - PubMed
-
- Eberhard BA, Sundel RP, Newburger JW, et al. Psoriatic eruption in Kawasaki disease. The Journal of Pediatrics. 2000;137:578–580. - PubMed
-
- Zvulunov A, Greenberg D, Cagnano E, et al. Development of psoriatic lesions during acute and convalescent phases of Kawasaki disease. J Paediatr Child Health. 2003;39:229–231. - PubMed
-
- Bayers S, Shulman ST, Paller AS. Kawasaki disease. Journal of American Dermatology. 2013;69:501.e1–501.e11. - PubMed
-
- Augustin M, Glaeske G, Radtke MA, et al. Epidemiology and comorbidity of psoriasis in children. Br J Dermatol. 2010;162:633–636. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
