

Dual antiplatelet therapy reduces stroke but increases bleeding at the time of carotid endarterectomy
- PMID: 26947237
- PMCID: PMC5065102
- DOI: 10.1016/j.jvs.2015.12.020
Dual antiplatelet therapy reduces stroke but increases bleeding at the time of carotid endarterectomy
Abstract
Objective: Controversy persists regarding the perioperative management of clopidogrel among patients undergoing carotid endarterectomy (CEA). This study examined the effect of preoperative dual antiplatelet therapy (aspirin and clopidogrel) on in-hospital CEA outcomes.
Methods: Patients undergoing CEA in the Vascular Quality Initiative were analyzed (2003-2014). Patients on clopidogrel and aspirin (dual therapy) were compared with patients taking aspirin alone preoperatively. Study outcomes included reoperation for bleeding and thrombotic complications defined as transient ischemic attack (TIA), stroke, or myocardial infarction. Secondary outcomes were in-hospital death and composite stroke/death. Univariate and multivariable analyses assessed differences in demographics and operative factors. Propensity score-matched cohorts were derived to control for subgroup heterogeneity.
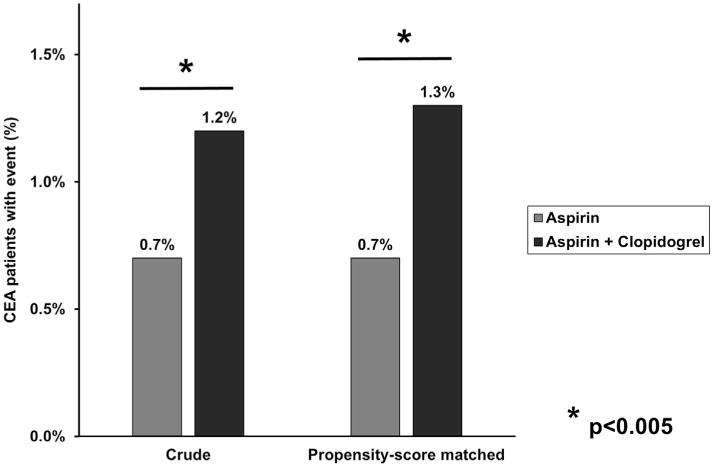
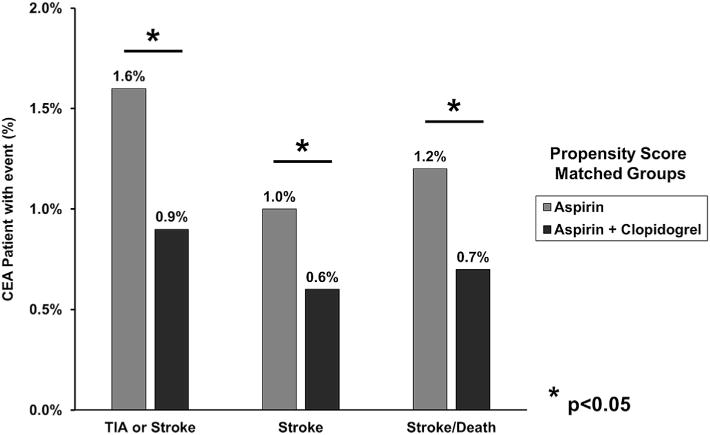
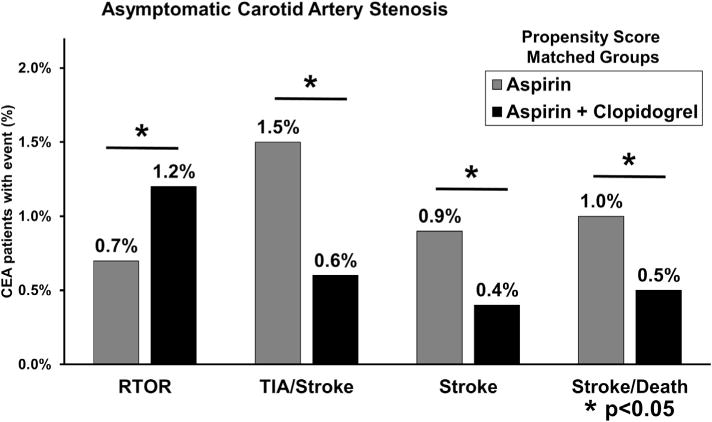
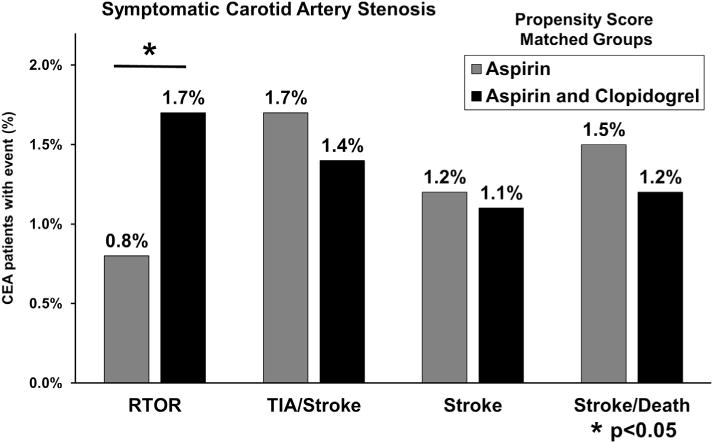
Results: Of 28,683 CEAs, 21,624 patients (75%) were on aspirin and 7059 (25%) were on dual therapy. Patients on dual therapy were more likely to have multiple comorbidities, including coronary artery disease (P < .001), congestive heart failure (P < .001), and diabetes (P < .001). Patients on dual therapy were also more likely to have a drain placed (P < .001) and receive protamine during CEA (P < .001). Multivariable analysis showed that dual therapy was independently associated with increased reoperation for bleeding (odds ratio [OR], 1.71; 95% confidence interval [CI], 1.20-2.42; P = .003) but was protective against TIA or stroke (OR, 0.61; 95% CI, 0.43-0.87; P = .007), stroke (OR, 0.63; 95% CI, 0.41-0.97; P = .03), and stroke/death (OR, 0.66; 95% CI, 0.44-0.98; P = .04). Propensity score matching yielded two groups of 4548 patients and showed that patients on dual therapy were more likely to require reoperation for bleeding (1.3% vs 0.7%; P = .004) but less likely to suffer TIA or stroke (0.9% vs 1.6%; P = .002), stroke (0.6% vs 1.0%; P = .04), or stroke/death (0.7% vs 1.2%; P = .03). Within the propensity score-matched groups, patients on dual therapy had increased rates of reoperation for bleeding regardless of carotid symptom status. However, asymptomatic patients on dual therapy demonstrated reduced rates of TIA or stroke (0.6% vs 1.5%; P < .001), stroke (0.4% vs 0.9%; P = .01), and composite stroke/death (0.5% vs 1.0%; P = .02). Among propensity score-matched patients with symptomatic carotid disease, these differences were not statistically significant.
Conclusions: Preoperative dual antiplatelet therapy was associated with a 40% risk reduction for neurologic events but also incurred a significant increased risk of reoperation for bleeding after CEA. Given its observed overall neurologic protective effect, continued dual antiplatelet therapy throughout the perioperative period is justified. Initiating dual therapy in all patients undergoing CEA may lead to decreased neurologic complication rates.
Copyright © 2016 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author conflict of interest: none. The editors and reviewers of this article have no relevant financial relationships to disclose per the JVS policy that requires reviewers to decline review of any manuscript for which they may have a conflict of interest.
Figures
Comment in
-
Discussion.J Vasc Surg. 2016 May;63(5):1270. doi: 10.1016/j.jvs.2015.12.022. Epub 2016 Mar 2. J Vasc Surg. 2016. PMID: 26947236 No abstract available.
-
Invited commentary.J Vasc Surg. 2016 May;63(5):1271. doi: 10.1016/j.jvs.2015.12.021. J Vasc Surg. 2016. PMID: 27109794 No abstract available.
References
-
- Hamish M, Gohel MS, Shepherd A, Howes NJ, Davies AH. Variations in the pharmacological management of patients treated with carotid endarterectomy: a survey of European vascular surgeons. Eur J Vasc Endovasc Surg. 2009;38:402–7. - PubMed
-
- Baracchini C, Gruppo M, Mazzalai F, Lorenzetti R, Meneghetti G, Ballotta E. Predictors of neck bleeding after eversion carotid endarterectomy. J Vasc Surg. 2011;54:699–705. - PubMed
-
- Saadeh C, Sfeir J. Discontinuation of preoperative clopidogrel is unnecessary in peripheral arterial surgery. J Vasc Surg. 2013;58:1586–92. - PubMed
-
- Morales Gisbert SM, Sala Almonacil VA, Zaragoza Garcia JM, Genoves Gasco B, Gomez Palones FJ, Ortiz Monzon E. Predictors of cervical bleeding after carotid endarterectomy. Ann Vasc Surg. 2014;28:366–74. - PubMed
-
- Payne DA, Twigg MW, Hayes PD, Naylor AR. Antiplatelet agents and risk factors for bleeding postcarotid endarterectomy. Ann Vasc Surg. 2010;24:900–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
