

Continuous Glucose Monitoring in Patients with Abnormal Glucose Tolerance during Pregnancy: A Case Series
- PMID: 26949348
- PMCID: PMC4767119
- DOI: 10.4137/JCM.S34825
Continuous Glucose Monitoring in Patients with Abnormal Glucose Tolerance during Pregnancy: A Case Series
Abstract
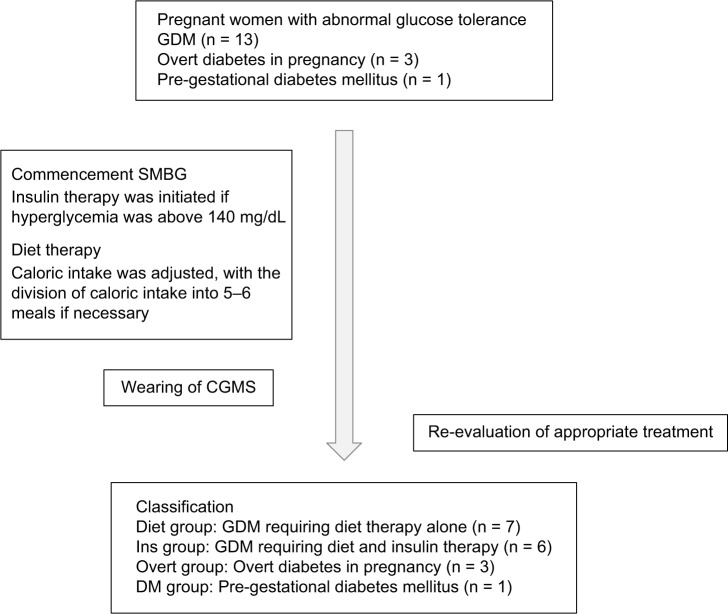
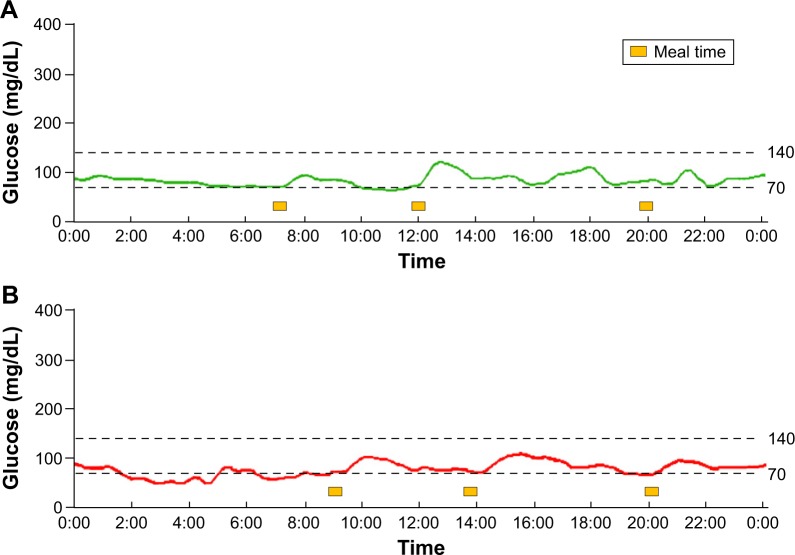
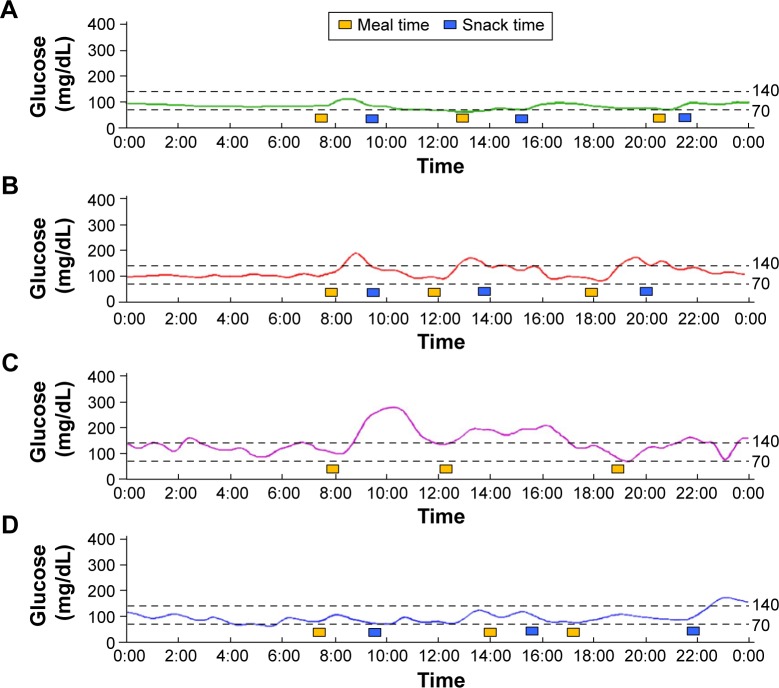
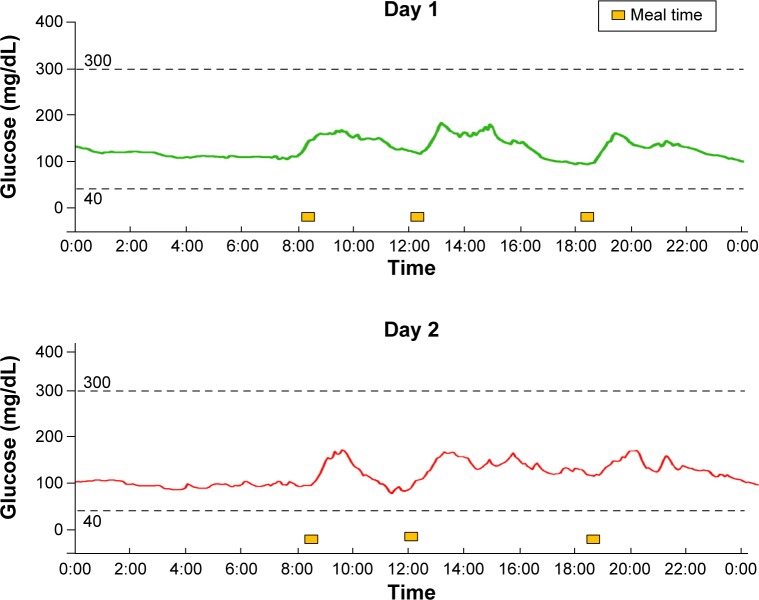
Abnormal glucose tolerance during pregnancy is associated with perinatal complications. We used continuous glucose monitoring (CGM) in pregnant women with glucose intolerance to achieve better glycemic control and to evaluate the maternal glucose fluctuations. We also used CGM in women without glucose intolerance (the control cases). Furthermore, the standard deviation (SD) and mean amplitude of glycemic excursions (MAGE) were calculated for each case. For the control cases, the glucose levels were tightly controlled within a very narrow range; however, the SD and MAGE values in pregnant women with glucose intolerance were relativity high, suggesting postprandial hyperglycemia. Our results demonstrate that pregnant women with glucose intolerance exhibited greater glucose fluctuations compared with the control cases. The use of CGM may help to improve our understanding of glycemic patterns and may have beneficial effects on perinatal glycemic control, such as the detection of postprandial hyperglycemia in pregnant women.
Keywords: continuous glucose monitoring; gestational diabetes mellitus; mean amplitude of glucose excursions; overt diabetes in pregnancy; pregestational diabetes.
Figures
References
-
- Norbert F. Banting lecture 1980. Of pregnancy and progeny. Diabetes. 1980;29:1006–1022. - PubMed
-
- Tsujino D, Nishimura R, Taki K, Miyashita Y, Morimoto A, Tajima N. Daily glucose profiles in Japanese people with normal glucose tolerance as assessed by continuous glucose monitoring. Diabetes Technol Ther. 2009;11(7):457–460. - PubMed
-
- Yariv Y, Ben-Haroush A, Chen R, Rosenn B, Hod M, Lager O. Diurnal glycemic profile in obese and normal weight nondiabetic pregnant women. Am J Obstet Gynecol. 2004;191:576–581. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
