

The Immunology of Neuromyelitis Optica-Current Knowledge, Clinical Implications, Controversies and Future Perspectives
- PMID: 26950113
- PMCID: PMC4813137
- DOI: 10.3390/ijms17030273
The Immunology of Neuromyelitis Optica-Current Knowledge, Clinical Implications, Controversies and Future Perspectives
Abstract
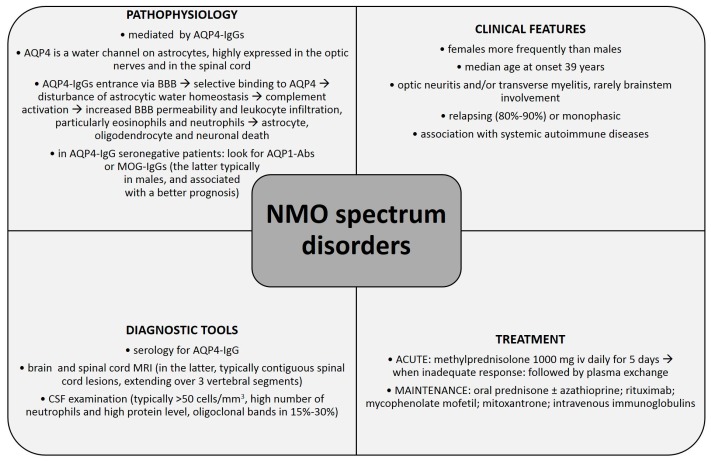
Neuromyelitis optica (NMO) is an autoimmune, demyelinating disorder of the central nervous system (CNS) with typical clinical manifestations of optic neuritis and acute transverse myelitis attacks. Previously believed to be a variant of multiple sclerosis (MS), it is now considered an independent disorder which needs to be differentiated from MS. The discovery of autoantibodies against aquaporin-4 (AQP4-IgGs) changed our understanding of NMO immunopathogenesis and revolutionized the diagnostic process. AQP4-IgG is currently regarded as a specific biomarker of NMO and NMO spectrum disorders (NMOsd) and a key factor in its pathogenesis. Nevertheless, AQP4-IgG seronegativity in 10%-25% of NMO patients suggests that there are several other factors involved in NMO immunopathogenesis, i.e., autoantibodies against aquaporin-1 (AQP1-Abs) and antibodies against myelin oligodendrocyte glycoprotein (MOG-IgGs). This manuscript reviews current knowledge about NMO immunopathogenesis, pointing out the controversial issues and showing potential directions for future research. Further efforts should be made to broaden our knowledge of NMO immunology which could have important implications for clinical practice, including the use of potential novel biomarkers to facilitate an early and accurate diagnosis, and modern treatment strategies improving long-term outcome of NMO patients.
Keywords: aquaporin-1 antibody (AQP1-Ab); aquaporin-4 immunoglobulin G (AQP4-IgG); immunopathogenesis; myelin oligodendrocyte glycoprotein immunoglobulin G (MOG-IgG); neuroimmunology; neuromyelitis optica (NMO); neuromyelitis optica spectrum disorder (NMOsd).
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
