

Improved Prediction of Drug-Induced Torsades de Pointes Through Simulations of Dynamics and Machine Learning Algorithms
- PMID: 26950176
- PMCID: PMC6375298
- DOI: 10.1002/cpt.367
Improved Prediction of Drug-Induced Torsades de Pointes Through Simulations of Dynamics and Machine Learning Algorithms
Abstract
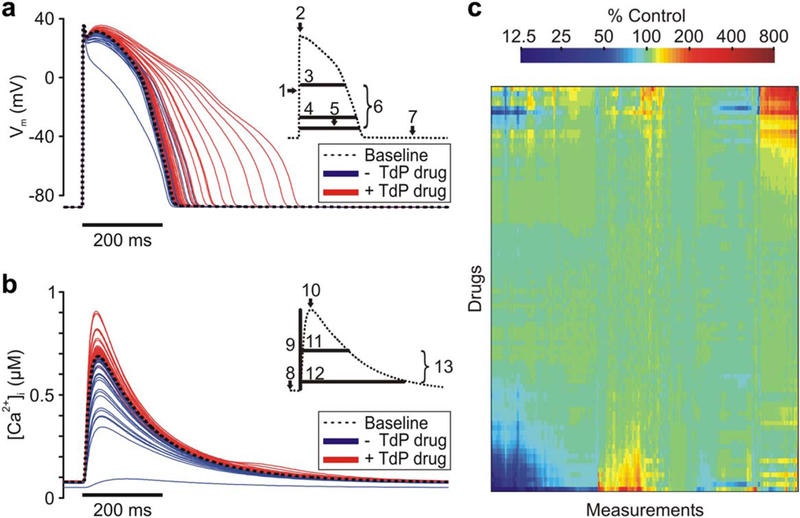
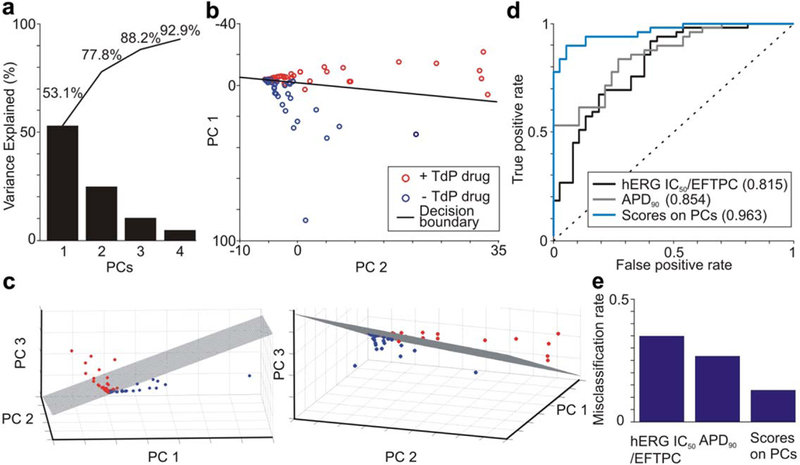
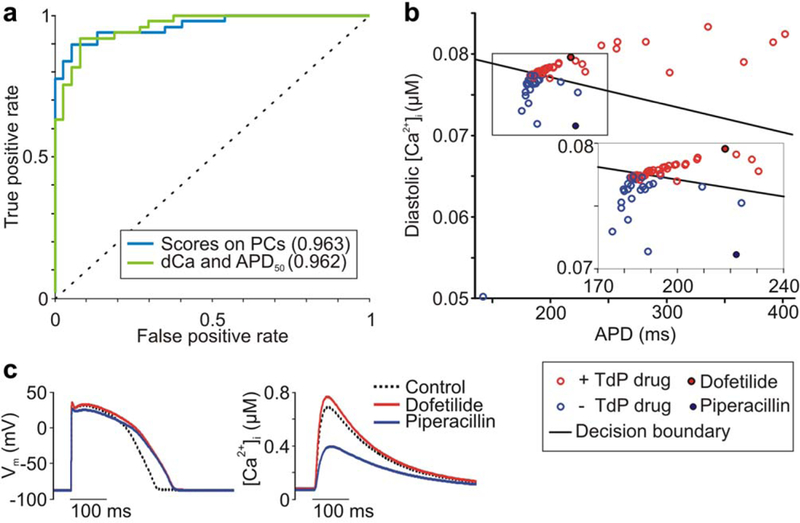
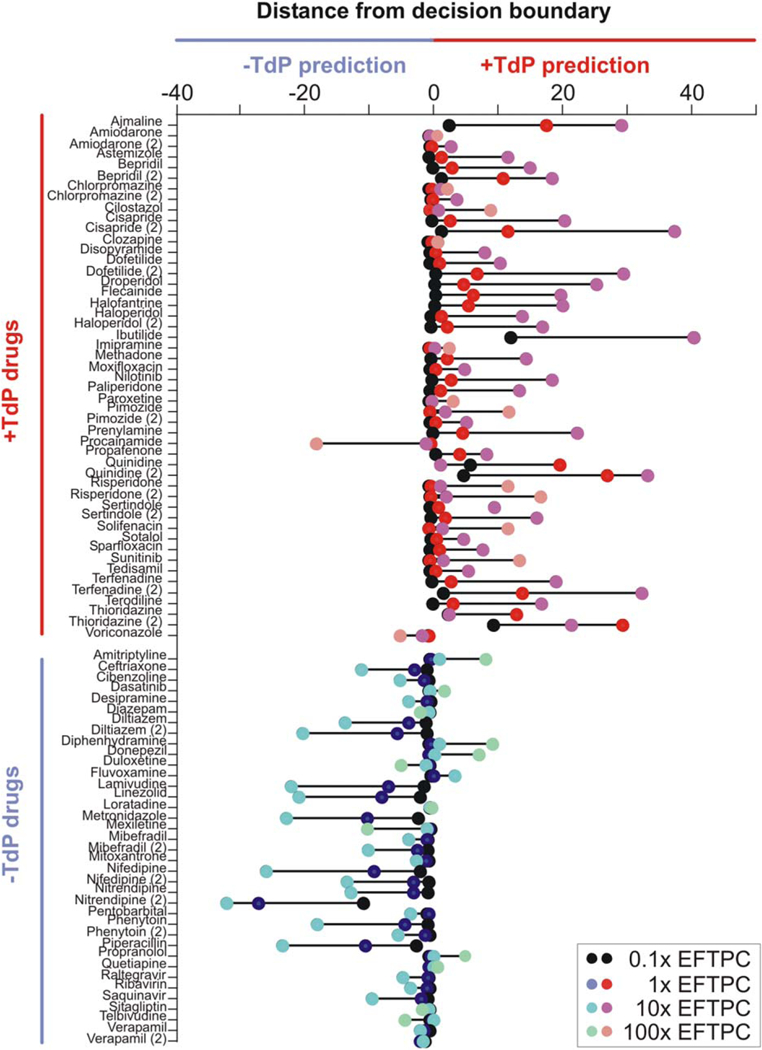
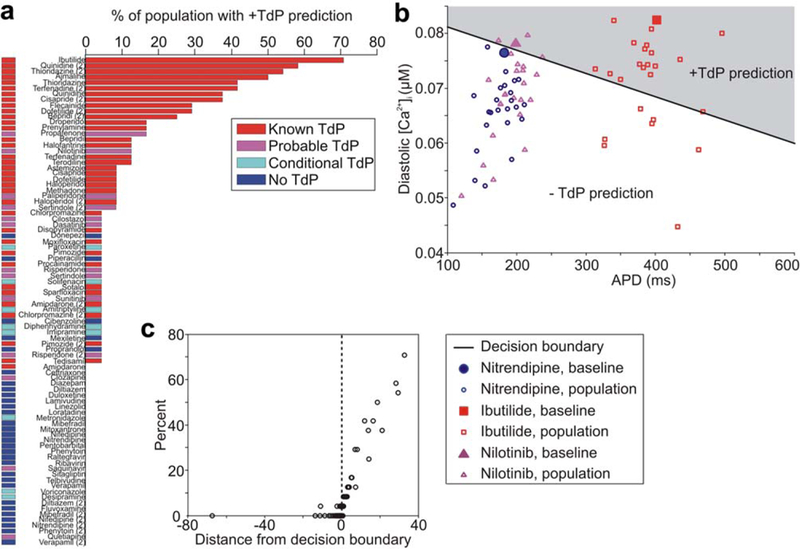
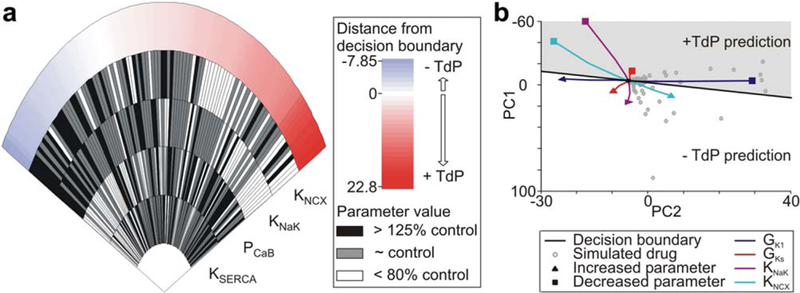
The ventricular arrhythmia Torsades de Pointes (TdP) is a common form of drug-induced cardiotoxicity, but prediction of this arrhythmia remains an unresolved issue in drug development. Current assays to evaluate arrhythmia risk are limited by poor specificity and a lack of mechanistic insight. We addressed this important unresolved issue through a novel computational approach that combined simulations of drug effects on dynamics with statistical analysis and machine-learning. Drugs that blocked multiple ion channels were simulated in ventricular myocyte models, and metrics computed from the action potential and intracellular (Ca(2+) ) waveform were used to construct classifiers that distinguished between arrhythmogenic and nonarrhythmogenic drugs. We found that: (1) these classifiers provide superior risk prediction; (2) drug-induced changes to both the action potential and intracellular (Ca(2+) ) influence risk; and (3) cardiac ion channels not typically assessed may significantly affect risk. Our algorithm demonstrates the value of systematic simulations in predicting pharmacological toxicity.
© 2016 The American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
CONFLICT OF INTEREST
The authors declared no conflict of interest.
Figures
Comment in
-
A new paradigm for predicting risk of Torsades de Pointes during drug development: Commentary on: "Improved prediction of drug-induced Torsades de Pointes through simulations of dynamics and machine learning algorithms".Clin Pharmacol Ther. 2016 Oct;100(4):324-6. doi: 10.1002/cpt.408. Epub 2016 Aug 1. Clin Pharmacol Ther. 2016. PMID: 27301674 Free PMC article.
-
Complexity vs. Simplicity: The Winner Is?Clin Pharmacol Ther. 2017 Mar;101(3):326. doi: 10.1002/cpt.503. Epub 2016 Sep 28. Clin Pharmacol Ther. 2017. PMID: 27617708 No abstract available.
-
Response to "Complexity vs. Simplicity: The Winner Is?" Mechanism-Based Classifiers Provide More Than Just Classification.Clin Pharmacol Ther. 2017 Mar;101(3):327. doi: 10.1002/cpt.500. Epub 2016 Nov 15. Clin Pharmacol Ther. 2017. PMID: 27618710 Free PMC article. No abstract available.
References
-
- Sanguinetti MC, Jiang C, Curran ME & Keating MT A mechanistic link between an inherited and an acquired cardiac arrhythmia: HERG encodes the IKr potassium channel. Cell 81, 299–307 (1995). - PubMed
-
- Food and Drug Administration, HHS. International Conference on Harmonisation; guidance on S7B nonclinical evaluation of the potential for delayed ventricular repolarization (QT interval prolongation) by human pharmaceuticals; availability. Notice. Fed. Regist. 70, 61133–61134 (2005). - PubMed
-
- Gintant G An evaluation of hERG current assay performance: translating preclinical safety studies to clinical QT prolongation. Pharmacol. Ther. 129, 109–119 (2011). - PubMed
-
- Redfern WS et al. Relationships between preclinical cardiac electrophysiology, clinical QT interval prolongation and torsade de pointes for a broad range of drugs: evidence for a provisional safety margin in drug development. Cardiovasc. Res. 58, 32–45 (2003). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
