

Algorithm-guided goal-directed haemodynamic therapy does not improve renal function after major abdominal surgery compared to good standard clinical care: a prospective randomised trial
- PMID: 26951105
- PMCID: PMC4782303
- DOI: 10.1186/s13054-016-1237-1
Algorithm-guided goal-directed haemodynamic therapy does not improve renal function after major abdominal surgery compared to good standard clinical care: a prospective randomised trial
Abstract
Background: Acute kidney injury is a common complication after major surgery. In this study, we investigated whether an algorithm-guided goal-directed haemodynamic therapy (GDT) can improve renal outcome compared to good standard clinical care.
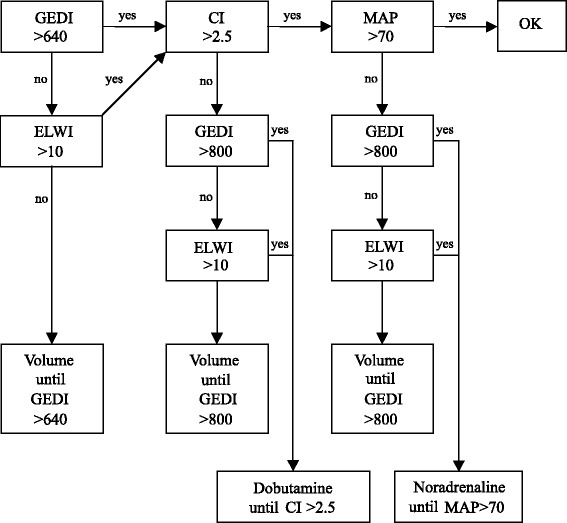
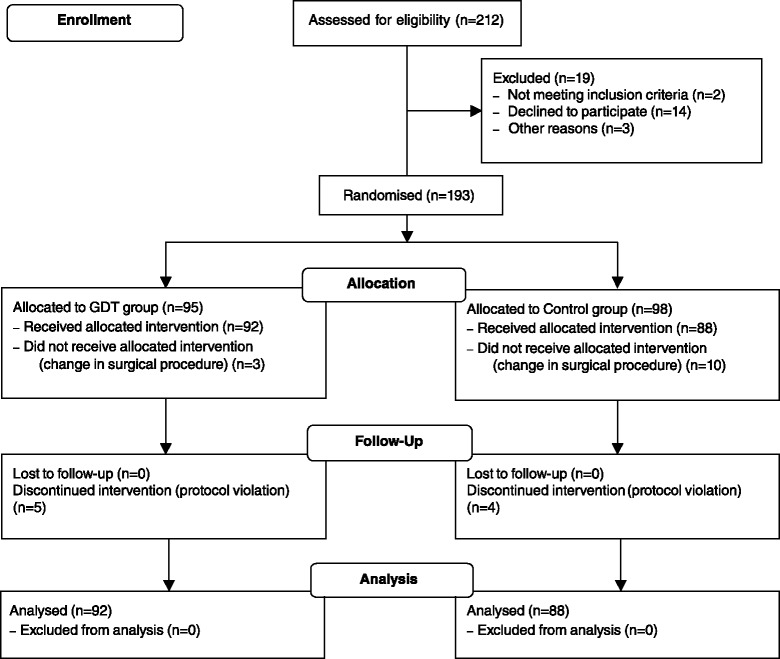
Methods: A total of 180 patients undergoing major abdominal surgery were prospectively and randomly assigned to one of two groups: in the GDT group, patients were treated with a GDT algorithm using transpulmonary thermodilution while standard care was applied to the control patients. Change in creatinine was studied as the primary end point, postoperative complications as well as 1-year mortality as secondary outcomes. Haemodynamics in GDT and control patients were compared calculating goal-achievement rates.
Results: Postoperative change in creatinine (18 ± 39 μmol/l (control) vs. 16 ± 42 μmol/l (GDT); mean difference (95 % confidence interval) 1.6 μmol/l (-10 to 13 μmol/l)) was comparable between the GDT and the control group. Postoperative complications and mortality during hospital stay and after 1 year were not influenced by the use of a GDT algorithm. Achievement rates of haemodynamic goals were not higher in the GDT group compared to the already high (>80 %) rates in the control group. Multivariate regression analysis revealed intraoperative hypotension (MAP < 70 mmHg) and postoperative hypovolaemia (GEDI < 640 ml/m(2)) as risk factors for postoperative renal impairment.
Conclusions: In this study, GDT was not superior to standard clinical care in order to avoid renal failure after major abdominal surgery. The reason for this finding is most likely the high achievement rate of haemodynamic goals in the control group, which cannot be improved by the GDT algorithm.
Trial registration: Clinicaltrials.gov; NCT01035541; registered 17 December 2009.
Figures
Comment in
-
Goal-directed therapy and acute kidney injury: as good as it gets?Crit Care. 2016 Jun 25;20(1):174. doi: 10.1186/s13054-016-1346-x. Crit Care. 2016. PMID: 27342646 Free PMC article.
Similar articles
-
The role of goal-directed therapy in the prevention of acute kidney injury after major gastrointestinal surgery: Substudy of the OPTIMISE trial.Eur J Anaesthesiol. 2019 Dec;36(12):924-932. doi: 10.1097/EJA.0000000000001104. Eur J Anaesthesiol. 2019. PMID: 31633603 Clinical Trial.
-
Oesophageal Doppler guided goal-directed haemodynamic therapy in thoracic surgery - a single centre randomized parallel-arm trial.Br J Anaesth. 2017 Jun 1;118(6):852-861. doi: 10.1093/bja/aew447. Br J Anaesth. 2017. PMID: 28575331 Clinical Trial.
-
Goal-directed fluid therapy in emergency abdominal surgery: a randomised multicentre trial.Br J Anaesth. 2021 Oct;127(4):521-531. doi: 10.1016/j.bja.2021.06.031. Epub 2021 Aug 11. Br J Anaesth. 2021. PMID: 34389168 Clinical Trial.
-
Hemodynamic goal-directed therapy and postoperative kidney injury: an updated meta-analysis with trial sequential analysis.Crit Care. 2019 Jun 26;23(1):232. doi: 10.1186/s13054-019-2516-4. Crit Care. 2019. PMID: 31242941 Free PMC article.
-
Meta-analysis of the effect of goal-directed therapy on bowel function after abdominal surgery.Br J Surg. 2015 May;102(6):577-89. doi: 10.1002/bjs.9747. Epub 2015 Mar 11. Br J Surg. 2015. PMID: 25759947 Review.
Cited by
-
Substitution of perioperative albumin deficiency disorders (SuperAdd) in adults undergoing vascular, abdominal, trauma, or orthopedic surgery: protocol for a randomized controlled trial.Trials. 2020 Aug 18;21(1):726. doi: 10.1186/s13063-020-04626-2. Trials. 2020. PMID: 32811539 Free PMC article.
-
Stroke volume variation and serum creatinine changes during abdominal aortic aneurysm surgery: a time-integrated analysis.J Nephrol. 2018 Aug;31(4):561-569. doi: 10.1007/s40620-018-0467-5. Epub 2018 Jan 17. J Nephrol. 2018. PMID: 29344813
-
Acute Kidney Injury in the Age of Enhanced Recovery Protocols.Dis Colon Rectum. 2018 Aug;61(8):946-954. doi: 10.1097/DCR.0000000000001059. Dis Colon Rectum. 2018. PMID: 29994959 Free PMC article.
-
Pulse Pressure Variation-Based Intraoperative Fluid Management Versus Traditional Fluid Management for Colon Cancer Patients Undergoing Open Mass Resection and Anastomosis: A Randomized Controlled Trial.Anesth Pain Med. 2023 Jul 23;13(4):e135659. doi: 10.5812/aapm-135659. eCollection 2023 Aug. Anesth Pain Med. 2023. PMID: 38024002 Free PMC article.
-
Impact of Enhanced Recovery After Surgery (ERAS) protocol versus standard of care on postoperative Acute Kidney Injury (AKI): A meta-analysis.PLoS One. 2021 May 20;16(5):e0251476. doi: 10.1371/journal.pone.0251476. eCollection 2021. PLoS One. 2021. PMID: 34015002 Free PMC article.
References
-
- O’Connor ME, Kirwan CJ, Pearse RM, Prowle JR. Incidence and associations of acute kidney injury after major abdominal surgery. Intensive Care Med. 2015. Epub ahead of print. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
