

An overview of the management of post-vasectomy pain syndrome
- PMID: 26952956
- PMCID: PMC4854072
- DOI: 10.4103/1008-682X.175090
An overview of the management of post-vasectomy pain syndrome
Abstract
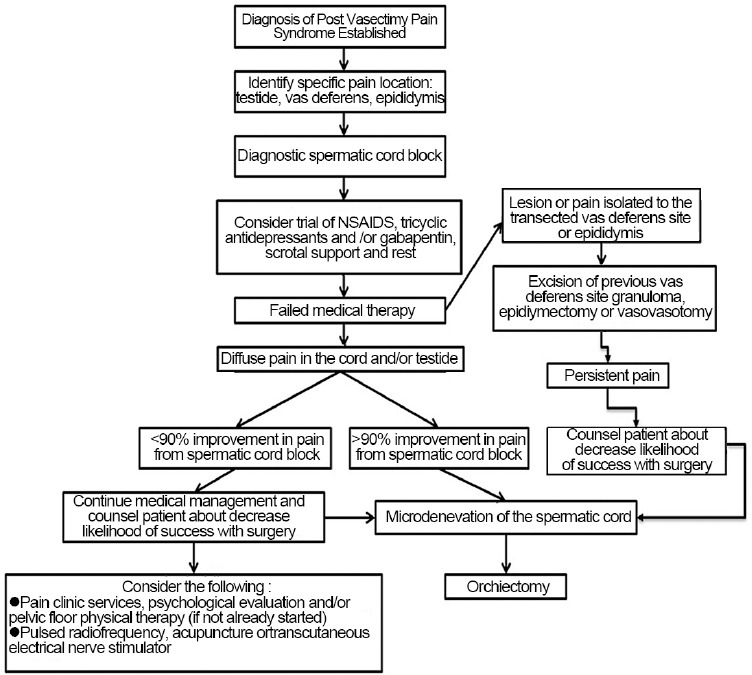
Post-vasectomy pain syndrome remains one of the more challenging urological problems to manage. This can be a frustrating process for both the patient and clinician as there is no well-recognized diagnostic regimen or reliable effective treatment. Many of these patients will end up seeing physicians across many disciplines, further frustrating them. The etiology of post-vasectomy pain syndrome is not clearly delineated. Postulations include damage to the scrotal and spermatic cord nerve structures via inflammatory effects of the immune system, back pressure effects in the obstructed vas and epididymis, vascular stasis, nerve impingement, or perineural fibrosis. Post-vasectomy pain syndrome is defined as at least 3 months of chronic or intermittent scrotal content pain. This article reviews the current understanding of post-vasectomy pain syndrome, theories behind its pathophysiology, evaluation pathways, and treatment options.
Figures
Comment in
-
Vasectomy reversal and other strategies to mitigate postvasectomy pain syndrome.Asian J Androl. 2016 May-Jun;18(3):338. doi: 10.4103/1008-682X.179243. Asian J Androl. 2016. PMID: 27056347 Free PMC article. No abstract available.
References
-
- Barone MA, Hutchinson PL, Johnson CH, Hsia J, Wheeler J. Vasectomy in the United States, 2002. J Urol. 2006;176:232–6. - PubMed
-
- Schwingl PJ, Guess HA. Safety and effectiveness of vasectomy. Fertil Steril. 2000;73:923–36. - PubMed
-
- Jamieson DJ, Costello C, Trussell J, Hillis SD, Marchbanks PA, et al. US collaborative review of sterilization working group. The risk of pregnancy after vasectomy. Obstet Gynecol. 2004;103:848–50. - PubMed
-
- Sharlip ID, Belker AM, Honig S, Labrecque M, Marmar JL, et al. American urological association. Vasectomy: AUA guideline. J Urol. 2012;188:2482–91. - PubMed
-
- Christiansen CG, Sandlow JI. Testicular pain following vasectomy: a review of postvasectomy pain syndrome. J Androl. 2003;24:293–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
