

Impact of vaginal parity and aging on the architectural design of pelvic floor muscles
- PMID: 26953079
- PMCID: PMC5003683
- DOI: 10.1016/j.ajog.2016.02.033
Impact of vaginal parity and aging on the architectural design of pelvic floor muscles
Abstract
Background: Vaginal delivery and aging are key risk factors for pelvic floor muscle dysfunction, which is a critical component of pelvic floor disorders. However, alterations in the pelvic floor muscle intrinsic structure that lead to muscle dysfunction because of childbirth and aging remain elusive.
Objectives: The purpose of this study was to determine the impact of vaginal deliveries and aging on human cadaveric pelvic floor muscle architecture, which is the strongest predictor of active muscle function.
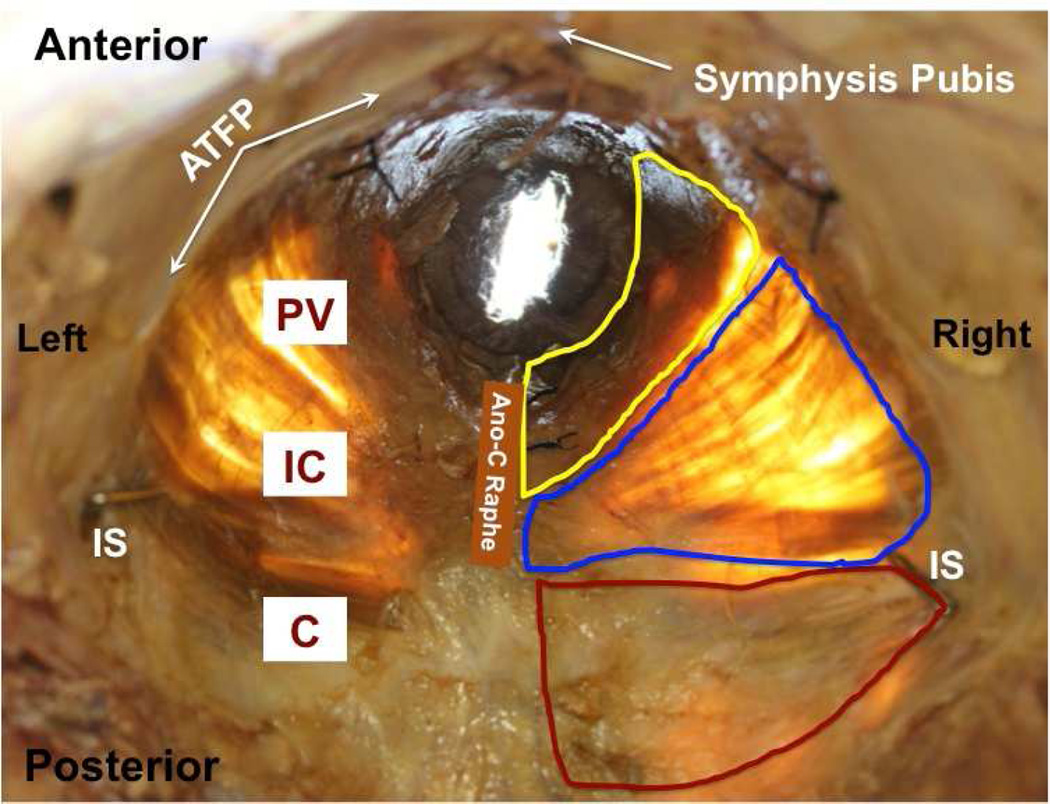
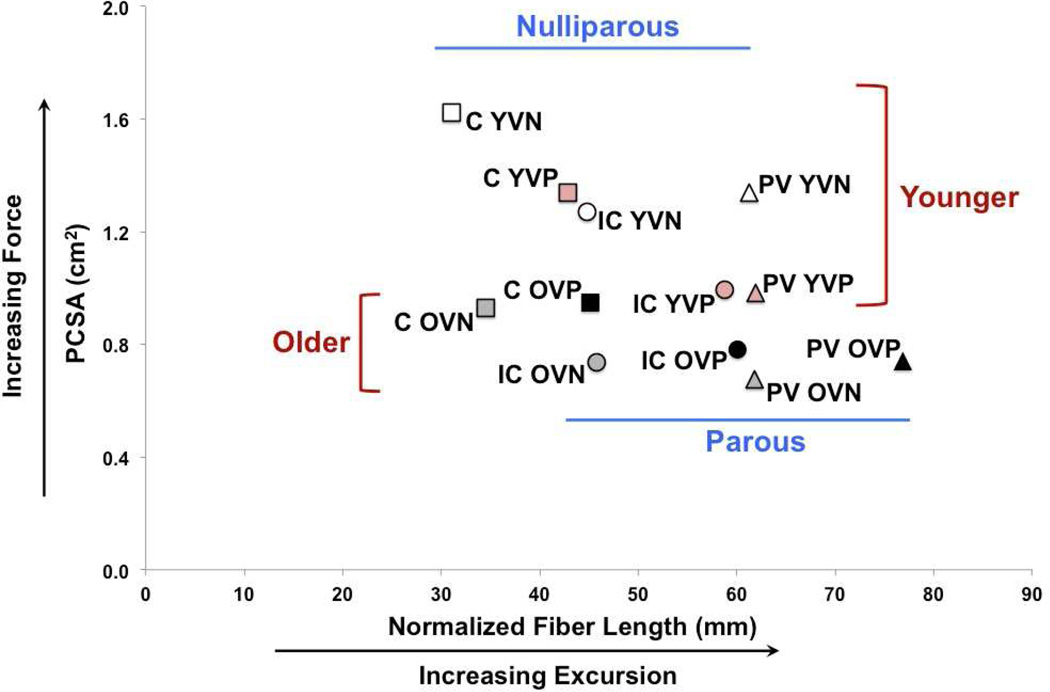
Study design: Coccygeus, iliococcygeus, and pubovisceralis were obtained from younger donors who were ≤51 years old, vaginally nulliparous (n = 5) and vaginally parous (n = 6) and older donors who were >51 years old, vaginally nulliparous (n = 6) and vaginally parous (n = 6), all of whom had no history of pelvic floor disorders. Architectural parameters, which are predictive of muscle's excursion and force-generating capacity, were determined with the use of validated methods. Intramuscular collagen content was quantified by hydroxyproline assay. Main effects of parity and aging and the interactions were determined with the use of 2-way analysis of variance, with Tukey's post-hoc testing and a significance level of .05.
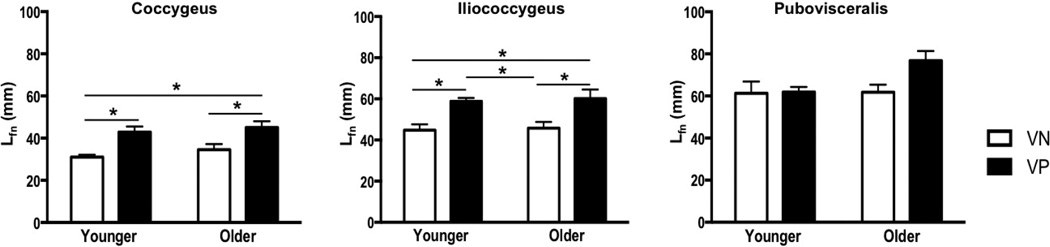
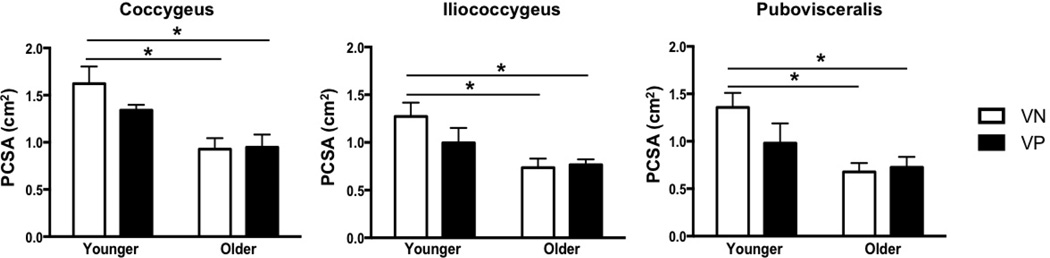
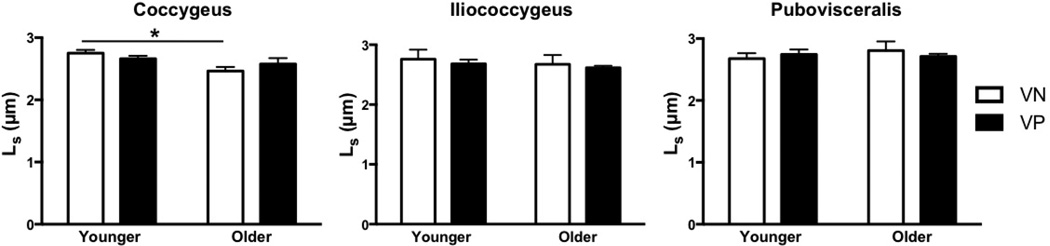
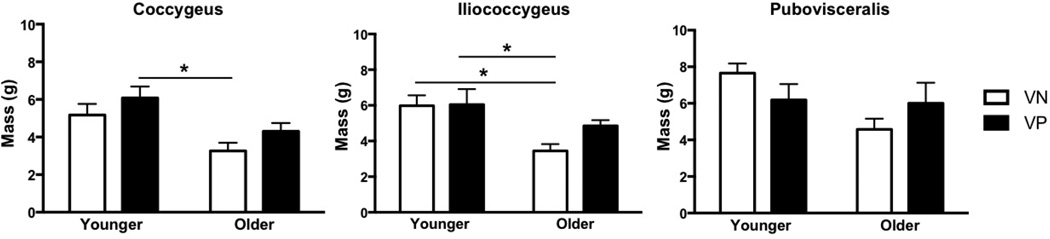
Results: The mean age of younger and older donors differed by approximately 40 years (P = .001) but was similar between nulliparous and parous donors within each age group (P > .9). The median parity was 2 (range, 1-3) in younger and older vaginally parous groups (P = .7). The main impact of parity was increased fiber length in the more proximal coccygeus (P = .03) and iliococcygeus (P = .04). Aging changes manifested as decreased physiologic cross-sectional area across all pelvic floor muscles (P < .05), which substantially exceeded the age-related decline in muscle mass. The physiologic cross-sectional area was lower in younger vaginally parous, compared with younger vaginally nulliparous, pelvic floor muscles; however, the differences did not reach statistical significance. Pelvic floor muscle collagen content was not altered by parity but increased dramatically with aging (P < .05).
Conclusions: Increased fiber length in more proximal pelvic floor muscles likely represents an adaptive response to the chronically increased load placed on these muscles by the displaced apical structures, presumably as a consequence of vaginal delivery. In younger specimens, a consistent trend towards decrease in force-generating capacity of all pelvic floor muscles in the parous group suggests a potential mechanism for clinically identified pelvic floor muscle weakness in vaginally parous women. The substantial decrease in predicted muscle force production and fibrosis with aging represent likely mechanisms for the pelvic floor muscle dysfunction in older women.
Keywords: aging; architecture; pelvic floor muscle; vaginal delivery.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflict of interest.
Figures
References
-
- DeLancey JOL. Pelvic Organ Prolapse: Clinical Management and Scientific Foundations. Clinical Obstetrics and Gynecology. 1993;36(4):895–896.
-
- Subak LL, Waetjen LE, van den Eeden S, Thom DH, Vittinghoff E, Brown JS. Cost of Pelvic Organ Prolapse Surgery in the United States. Obstetrics & Gynecology. 2001;98(4) - PubMed
-
- Wilson L, Brown JS, Shin GP, Luc K-O, Subak LL. Annual Direct Cost of Urinary Incontinence. Obstetrics & Gynecology. 2001;98(3) - PubMed
-
- Gregory WT, Nygaard I. Childbirth and Pelvic Floor Disorders. Clinical Obstetrics and Gynecology. 2004;47(2):394–403. - PubMed
-
- Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of Surgically Managed Pelvic Organ Prolapse and Urinary Incontinence. Obstetrics & Gynecology. 1997;89(4):501–506. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
