

The Hypoglycemic Phenotype Is Islet Cell-Autonomous in Short-Chain Hydroxyacyl-CoA Dehydrogenase-Deficient Mice
- PMID: 26953163
- PMCID: PMC4878426
- DOI: 10.2337/db15-1475
The Hypoglycemic Phenotype Is Islet Cell-Autonomous in Short-Chain Hydroxyacyl-CoA Dehydrogenase-Deficient Mice
Abstract
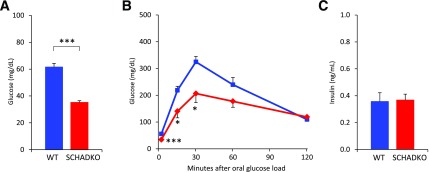
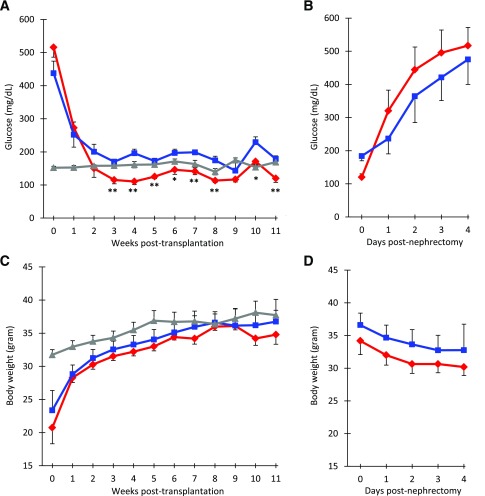
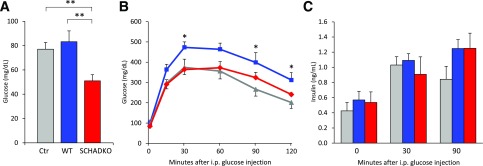
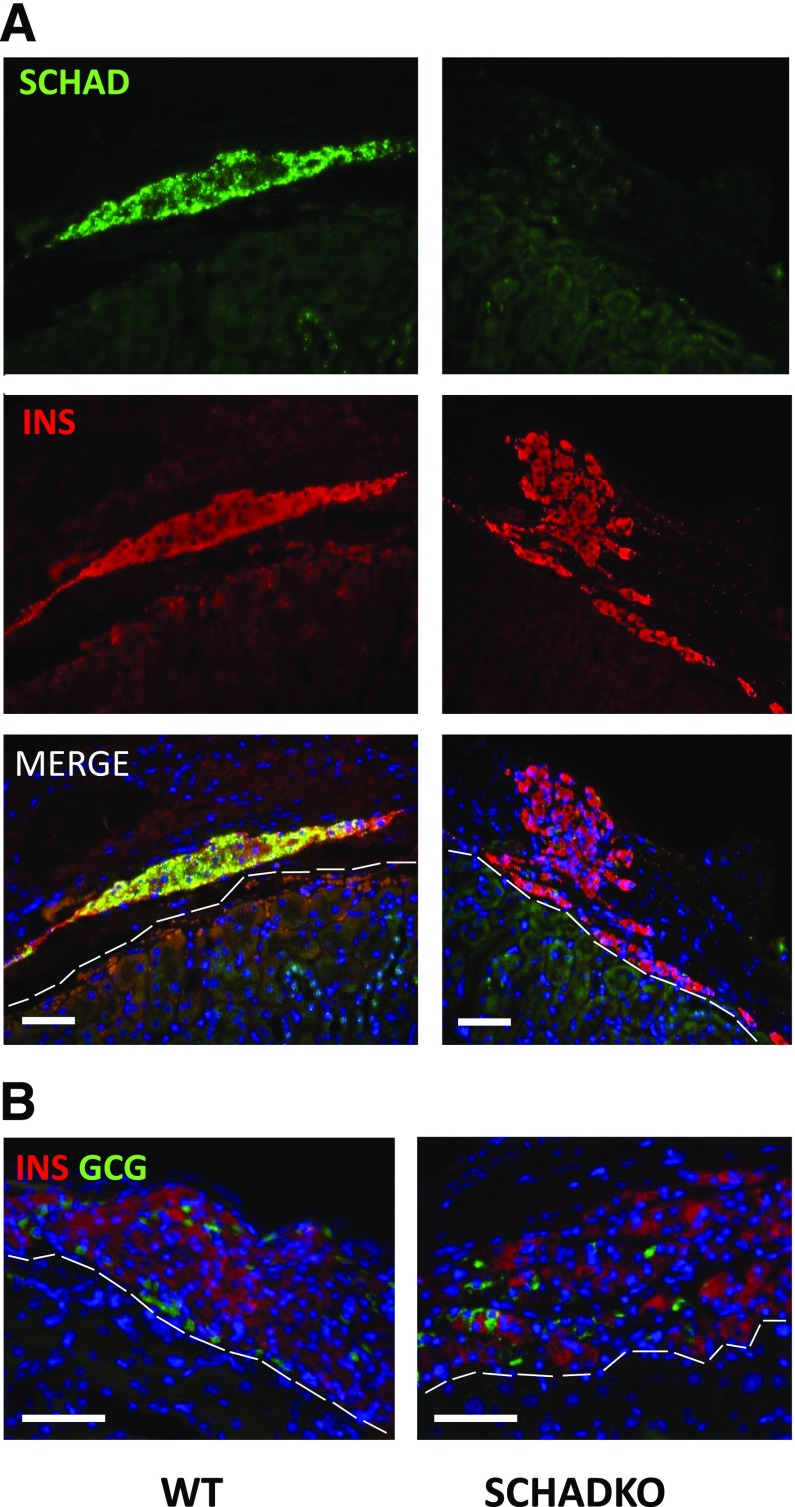
Congenital hyperinsulinism of infancy (CHI) can be caused by inactivating mutations in the gene encoding short-chain 3-hydroxyacyl-CoA dehydrogenase (SCHAD), a ubiquitously expressed enzyme involved in fatty acid oxidation. The hypersecretion of insulin may be explained by a loss of interaction between SCHAD and glutamate dehydrogenase in the pancreatic β-cells. However, there is also a general accumulation of metabolites specific for the enzymatic defect in affected individuals. It remains to be explored whether hypoglycemia in SCHAD CHI can be uncoupled from the systemic effect on fatty acid oxidation. We therefore transplanted islets from global SCHAD knockout (SCHADKO) mice into mice with streptozotocin-induced diabetes. After transplantation, SCHADKO islet recipients exhibited significantly lower random and fasting blood glucose compared with mice transplanted with normal islets or nondiabetic, nontransplanted controls. Furthermore, intraperitoneal glucose tolerance was improved in animals receiving SCHADKO islets compared with those receiving normal islets. Graft β-cell proliferation and apoptosis rates were similar in the two transplantation groups. We conclude that hypoglycemia in SCHAD-CHI is islet cell-autonomous.
© 2016 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures
References
-
- Kapoor RR, James C, Hussain K. Advances in the diagnosis and management of hyperinsulinemic hypoglycemia. Nat Clin Pract Endocrinol Metab 2009;5:101–112 - PubMed
-
- Rahman SA, Nessa A, Hussain K. Molecular mechanisms of congenital hyperinsulinism. J Mol Endocrinol 2015;54:R119–R129 - PubMed
-
- Sandal T, Laborie LB, Brusgaard K, et al. . The spectrum of ABCC8 mutations in Norwegian patients with congenital hyperinsulinism of infancy. Clin Genet 2009;75:440–448 - PubMed
-
- Molven A, Matre GE, Duran M, et al. . Familial hyperinsulinemic hypoglycemia caused by a defect in the SCHAD enzyme of mitochondrial fatty acid oxidation. Diabetes 2004;53:221–227 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
